Using eastern medicine and traditions to combat period discomfort
If you have difficult periods, you’ve probably searched high and low for real and lasting relief. We talked with acupuncturist and Chinese Medicine practitioner Adam Burrill about remedies that have proven useful for many women for centuries. Turns out, what we eat can have significant effectsasgood and badason how we feel, particularly during our periods or times of hormonal change. Here’s what Adam had to share.
From Adam Burrill, L.Ac., MSOM:
Many women experience difficult periods in their teens, during stressful times, or as they approach menopause.
Symptoms women experience vary widely but can include cramping, irritability, back/hip soreness, headaches, digestive disturbance, fatigue, general discomfort, breast tenderness, sleeplessness and more.
Don’t despair: These symptoms may be avoidable.
If you go to your doctor to complain about symptoms related to your periods, the first thing your doctor is likely to give you is birth control. The birth control pill, and other birth control that contains hormones (like injectable forms or some IUDs), is likely to change your cycle by dominating the hormonal communication that is going on in your body to signal creation of estrogen, progesterone, and other hormones. The logic here is that your body must be regulating your cycle improperly. Sometimes these extra hormones work to relieve undesirable symptoms; sometimes they don’t.
Seeking relief in Chinese Medicine
Chinese Medicine, of which acupuncture is the most famous component, offers some perspective on the menstrual cycle that may be helpful.* Chinese Medicine was developed over many centuries of scientific observation, but uses a different kind of logic than mainstream medicine does today.
In Chinese Medicine, the menstrual cycle is governed by the blood. The healthy state of your blood produces healthy fertility and menses. Those essential things we sometimes neglect”decent sleep, minimal stress and a proper diet, for example”can affect your blood and lead to worse periods. Some things to avoid: excessive alcohol, sugar, caffeine and tobacco.
The four basic patterns of problem periods
There are four basic patterns we see with difficult periods: The healthy state of your blood (from the Chinese Medicine perspective) can be affected by stagnation of circulation, emotional stagnation, lack of nutrients, and high stress levels.
With circulatory or emotional stagnation, you may experience cramps, back soreness and emotional upset, and you may see menstrual blood that is dark red or brown with clots. For relief, eat more spicy foods with herbs like cumin, coriander, cinnamon, oregano, and turmeric in them and increase the amount of exercise you get.
If you’re lacking nutrients, you may observe menstrual blood that is thin and a flow that lasts only one or two days with cramping, hot flashes, and fatigue during and following menses. For relief, eat lots of vegetables, healthy proteins and fats, get lots of rest, and don’t exercise excessively.
If you’re frequently under a lot of stress, you may experience any of the above. Try to reduce your stress and take all of the advice above. You can also go to an acupuncturist; acupuncture and herbs can smooth out your cycle fairly quickly.
*These are general guidelines and are not meant to diagnose or cure any disease. If you have serious problems, please see a licensed practitioner or your doctor.
Adam Burrill, L.Ac., MSOM, is an acupuncturist at Spring and Autumn Acupuncture in Portland, Oregon. Adam specializes in pain conditions and sports medicine and helps patients with stress, anxiety, depression, women’s health concerns, and neurological disorders.
That’s the most common question we hear from women as they come to Gennev for answers and solutions for the perimenopause and post-menopause symptoms they’re experiencing.
“I’m growing chin-hairs, is that normal?”
“I just can’t focus at work anymore. Is that normal, or am I losing my edge?”
“I lash out at my husband and kids for no reason. Am I going crazy?”
“Is it normal to have burning ears and face during a hot flash, along with an increased heart rate at the same time?”
These are a few questions I’ve heard from our Gennev community as either face to face, in email or in the Gennev Facebook community Midlife & Menopause Solutions.
It’s normal to want to know if something is normal when it’s fresh, new and mostly discomforting.
I’m thrilled to see women putting themselves out there and asking questions.
Most of the time the changes are normal; other times they’re not.
One of my favorite articles published on gennev.com is Menopause education and knowing the edges of “normal.” It’s a story about Ann, a woman who knew something wasn’t normal and she was scared, but all signs pointed to normalcy.
She kept pressing and finally got an answer. When she approached us to tell her story, we knew there had to be other women out there who were asking “is this normal” and not getting the help they needed.
Yesterday I was interviewed by a journalist doing a story on menopause in Hollywood. She asked if I thought that it was “normalizing,” and I said yes.
In the last six months, more articles have been published on menopause in the workplace, the cost of hormone prescriptions, and the social norms of middle-aged women in 2019.
These conversations are chipping away at normalizing women’s reproductive health and the beautiful cycle that is life. Even more, the growing awareness improves women’s understanding of what is normal and what’s not.
Even Gwyneth Paltrow is hot on the topic. Whether you’re a Gwyneth fan or not, the fact that she’s talking about menopause is good for all of us. It raises its awareness. I don’t necessarily agree with all of her approaches, but I appreciate that she’s putting herself out there to share her experience and try to move the needle on how society treats menopause’s place in women’s lives.
So, keep asking if changes in your body are normal. It’s the first step to taking control of your health.
And if you have no one to ask, then inquire with us at Gennev. We’re in the business of getting you the answers that you deserve.



“
“
“
“
Back in May of 2017, we spoke with Dr. Lora Shahine of Pacific NW Fertility about fertility, in vitro fertilization, the stigma of miscarriage, and having hope.
Interview With Lorna Marshall of Pacific NW Fertility
The podcast was so popular, we returned to the clinic to talk with one of Dr. Shahine’s colleagues, Dr. Lorna Marshall, about another fertility preserving option: egg freezing. Once reserved for women about to undergo cancer treatments that would destroy their ovaries, egg freezing has become a popular way for healthy, younger women to delay pregnancy while pursuing a career.
Dr. Marshall is a practicing specialist in Reproductive Endocrinology and Infertility, serving the Seattle community for over 25 years. In this first part of our two-part podcast, Dr. Marshall spoke with us about the history and science behind freezing eggs. We’ve been freezing sperm for ages; why did it take so long to learn to freeze an egg, and what are the risks?
For the answer to that and other questions, listen up:
1:22 as Getting into the egg freezing business
How does one become a reproductive endocrinologist/fertility specialist? For Dr. Marshall, her medical career paralleled the history of IVF, so it must have been destiny, she says. She shares her story of how her interest in fertility medicine grew as the science, ethics, and practice got more and more fascinating.
2:29 as How IVF got interesting
At first, fertility was uninteresting to her, Dr. Marshall says. The success rates were low, there wasn’t much doctors could do to help. Then IVF started to get really interesting”¦
4:42 as The biggest barrier to fertility treatments
Have patients changed over time? Not so much, Dr. Marshall says; they’re still “everyday folks.” But formerly couples came in only after they’d been trying for a very long time. Nowadays, couples are willing to try a more complicated route sooner. The big barrier to fertility treatments hasn’t changed: money.
6:54 as How have fertility patients changed?
In the past, Dr. Marshall says, fertilization specialists dealt almost entirely with couples who were infertile. Now, they have a whole separate clientele of women and couples who are looking for ways to postpone pregnancy.
7:51 as Egg freezing is still a new science: what docs are learning
We were curious to know what a woman who elects for fertility preservation looks like. Being able to elect for egg freezing is very new, Dr. Marshall says, only around since 2012. So we’re still discovering what women might want this option.
9:57 as The history and science of freezing eggs (and other things)
So what makes eggs so darn hard to freeze, compared to an embryo? Dr. Marshall explains how, previously, egg freezing was reserved for women who had received a cancer diagnosis and would likely be infertile after treatment. Such a small audience meant there wasn’t much opportunity to learn, and that slowed advancement of techniques.
13:08 as Is egg freezing “experimental”?
Professional societies considered freezing eggs “experimental” until January 2013, finally lifting the designation because enough successes had been recorded. Four years later, egg freezing is still not advised as an elective procedure, just for cancer patients or for other special circumstances.
14:54 as No regrets for those who didn’t freeze their eggs 20 years ago
For anyone who might feel regret for not having chosen an egg-freezing option when they were younger, Dr. Marshall is quick to reassure them that it would not have been possible. “No regrets,” she says. All those fortunate celebrities getting pregnant at 50 probably aren’t doing it with their own eggs.
In part 2, “fertility planning and egg freezing with Dr. Lorna Marshall,” Jill and Dr. Marshall talk more about the women who are electing to freeze their eggs as a way of postponing as but still having the option of as pregnancy and family, using their own eggs. Hear about global corporations offering egg freezing as a “benefit” to female employees and how society’s approach to fertility is changing.
If you’re looking for more information about fertility and options for family planning, you can visit Dr. Marshall and her colleagues at Pacific NW Fertility.
Would you consider freezing your eggs in order to delay pregnancy? Why or why not? We’d love to hear your thoughts; please share in the comments section, email us at info@gennev.com, or let us know on Gennev’s Facebook page or in Midlife & Menopause Solutions, Gennev’s closed Facebook group.
Some women find relief from headaches after menopause; some find the headaches are worse and more frequent, especially in the years leading up to menopause. Some women may find themselves having migraines for the first time ever. [Read Kara’s story of migraines, hormones and pregnancy.]
So, can menopause cause headaches? Well, Around 60% of women in perimenopause and menopause report new or increased head pain. That would strongly indicate “yes.”
Why menopause headaches happen (or stop happening)
Estrogen and progesterone drop just before your period starts, so women whose headaches are triggered by hormone withdrawal (who knew that was a thing?) may find head pain intensifies in perimenopause when hormone levels are fluctuating and declining overall. The good news is, hormonal headaches generally decline or stop altogether after menopause. They can also be caused by high blood pressure, and at times heart palpitations, both of which can onset during menopause.
When to consult a doctor
If your headaches are worse and start to interfere with your life, see a doctor. Yes, changes are normal during this time when everything is changing, but a doc can determine if what you’re experiencing needs medical intervention. Further, a health care professional who specializes in headaches and migraines can help you identify triggers and establish a treatment plan.
If headaches are interfering with your day-to-day life, a Gennev menopause-certified gynecologist can give you a trusted opinion, determine if medication is right for you, and they can provide prescription support. Book an appointment with a doctor here.
Treatment for menopause headaches
The solution may depend on the trigger. Generally, if the reduction in hormones triggers headaches, low-dose birth control pills may provide some relief.
Hormone replacement therapy (HRT) can also help level out hormones during the transition of perimenopause and into menopause, but because triggers and responses are so unique, women should work closely with their doctors to get the treatments right, including dosage and how the treatment is delivered. Also, perimenopause isn’t a time of consistent, dependable decline, so monitoring closely and shifting treatments accordingly will be necessary for many women.
For women with a history of breast cancer or blood clots, HRT may not be the treatment route of choice. In that case, there are several paths that can help.
Identify and banish triggers
Specialists often recommend that those with head pain keep a food and drink journal for several months. This can help identify triggers so they can be eliminated from your diet. (Spoiler alert: coffee, wine, chocolate, and some cheeses are common triggers. We know, bummer.)
Use alternative pain-management strategies
Biofeedback, acupuncture, and relaxation techniques have shown promise in helping people reduce and manage all kinds of pain, including headaches. How long do your menopause headaches last?
Lifestyle changes
Menopausal head and neck pain can be greatly improved by regular, consistent sleep patterns; exercise can help your body relax and promote better sleep and circulation; water retention may be partly responsible for your head pain, so reducing salt and hydrating are good things to try. Cut out smoking, of course, if you possibly can. I found that better eye care helped me: I needed to move to reading glasses, plus my eyes are dryer now. The constant squinting and strain were making headaches worse and getting the right prescription and some over-the-counter drops helped enormously. And I got a nice big monitor that is easier to see and a better ergonomic fit than looking down at my laptop. See? Lifestyle changes. They actually do help.
CBD
Many women find real relief with CBD oil. While science hasn’t yet determined why CBD helps with pain, there is certainly lots of anecdotal evidence that it does, so you may want to give it a try.
It’s frustrating, we know: headaches may get better, they may get worse. Hormones may help or hurt. Menopause could mean the end of migraines or the beginning. Whatever you experience, there is help. And making good lifestyle changes like getting regular sleep, drinking more water, and exercising in the fresh air certainly won’t hurt you.
We’d Love To Hear About Your Menopause And Headache Stories
We’d love to know if you’ve experienced changes. Even if you’re not perimenopausal, what’s your experience with head pain? Every voice or menopause story adds to the conversation, so please join in in the comments or on Facebook or Twitter.
“
The information on the Gennev site is never meant to replace the care of a qualified medical professional. Hormonal shifts throughout menopause can prompt a lot of changes in your body, and simply assuming something is “just menopause” can leave you vulnerable to other possible causes. Always consult with your physician or schedule an appointment with one of Gennev’s telemedicine doctors before beginning any new treatment or therapy.
“
“
Weight gain in the menopause transition is one of the most common complaints we hear about at Gennev.
And there’s good reason for concern.
According to an an article published by the North American Menopause Society, “about two-thirds of women ages 40 to 59 and nearly three-quarters of women older than 60 are overweight (body mass index [BMI] greater than 25 kg/m2). On average, midlife women gain 1.5 pounds (0.7 kg) per year.” Menopause weight management is simply tougher.
Why does it matter? Honestly, we think you’re beautiful at any size, but there are health complications that can accompany weight gain, particularly when that weight accumulates around the midsection.
But managing weight as like so many things as is a real challenge in your transition. Fatigue in menopause makes it harder to exercise. Life complications and self-consciousness may keep us from going to the gym. And to make things harder, appetite often ramps up, making healthy eating harder.
For help, we turned to our doctors of physical therapy, Dr. Meagan Peeters-Gebler and Dr. Brianna Droessler-Aschliman. We asked: Diets are pretty universally horrible, it’s pretty hard to exercise the excess weight away as does anything work?
Yes, they said, but it’s a pretty different mindset and approach than most of us are used to when it comes to managing our weight: Practice mindfulness.
Menopause Weight Management: Mindfulness
For the purposes of this conversation, “mindfulness” means paying attention. Not doing things distractedly while thinking of the eight other things you’ve got to do, but instead focusing fully on the moment.
Employing a mindful approach to every aspect of eating takes practice and effort, but the benefits are many.
Meal planning
When health issues interfered with life-as-usual, Meagan and her family got into a routine of planning an entire month’s worth of meals. They map out events, who’s home, who’s gone, etc., then fill in the blocks as an entire month’s worth of dinners, with leftovers for lunches.
And it really works. Seeing the whole month, they’re able to see if their diet is diverse, nutritionally complete, and satisfying. According to Meagan, “We can see we’re getting at least one fish, one turkey, one chicken, one red meat, one vegetarian, one meal out, maybe, and at least one new recipe.”
“When you map it out, it becomes non-negotiable,” Meagan says. “And when you make a plan, eating becomes a mindful choice, not a binging, emotional, blood-sugar-drop, had-a-bad-day-at-work-where-are-the-chocolate-chip-cookies impulse decision. We have all five years’ worth of meals with recipes and shopping lists; now it takes less than 15 minutes to plan for the whole month.”
It took a couple months of taking the time and being really mindful and attentive, but now it’s incredibly efficient, and they’ve reduced cost, waste, and stress. And of course, they’re eating more healthfully because they’re paying attention.
Shopping and meal prep
Brianna and her husband lead busy lives, so food and meals need to fit their lifestyle. Meal prep beforehand helps them control what they eat and also limits stress on hectic mornings.
“If we don’t have lunches prepped, we can tell the difference. We’re just grabbing things out of the refrigerator and hoping it’s good when lunchtime rolls around. But when it’s all laid out in advance, we can see if we have protein, if we have the right combination of veggies, if we’ve remembered to add in some fruit.”
Not being at the mercy of the cafeteria or local fast food offerings makes weight management and nutrition a whole lot easier.
And knowing what you’re going to prepare makes shopping exponentially easier, says Bri. They make a list and stick to it, meaning no impulse buys. They know exactly what to buy and how much, so they don’t spend extra money or buy food that ultimately gets wasted.
Being open to experimenting can also be a way to approach food more mindfully. Meagan says she was upset with her Brussels-sprouts hating mom when she discovered how delicious a sprout roasted with balsamic vinegar and olive oil could be!
While you’re being mindful of what you’re buying, you might also consider where. As we enter spring and summer in the US, farmers’ markets and produce stands fill up with awesome local fruits and veggies, Bri reminds us. Farm-fresh food often retains more nutrients than produce that’s been sitting in warehouses or travelling, so shopping at a market can boost the value of the foods you’re buying.
Eating
Finally, actually consuming food should be an act of mindfulness. I think most of us have experienced that feeling of sitting on the couch with some chips or crackers, only to find, when the show is over, that we’ve eaten the whole bag or tube.
First, be aware of what you’re putting in your mouth, food or liquid. If you have an impulse or habit, you may end up eating or drinking things that aren’t as nutritious. “If you have a soda in your hand, put it down,” Meagan says. “We tend to grab what’s convenient and handy, but give yourself a moment to think about it. Do I really want this sugary soda? That may be all the time you need to make a better choice.”
Tune into your body’s signals: are you really hungry at all? Meagan’s husband keeps an apple on his desk: if he’s hungry, he can eat the apple. If the apple isn’t all that tempting, he knows he’s not really hungry. Maybe you’re thirsty, Meagan says. “A lot of time people think they’re hungry when they’re really thirsty, so get a drink of water first, then decide about food.”
Pay attention. Smell all the gorgeous scents; really take in the rich array of colors; taste every bite in all its complexity. And chew. Like, really chew. The action of chewing your food thoroughly activates processes in the body that break down food better and make it more available to your body as nutrition.
Also, eating more slowly gives your body a chance to signal when it’s had enough. It takes time for satiety signals to get to your brain, Bri reminds us, so slow down. That can be hard if, like Bri, you grew up with siblings and eating fast was the only way to ensure you got your share, she says!
Change
Now that you’re tuned in to what you’re eating, it’s time to make changes. But don’t try to make all the changes at once. Go down a size at Starbucks, from a vente to a grande (grande to vente? Whatever, you get it). Replace one soda a day with a flavored water. Do the apple trick to determine if you’re hungry or if the impulse is coming from somewhere else.
“Don’t get obsessed with perfection,” Bri reminds us. “That just sets you up for failure. If you made a less-healthy decision today, don’t beat yourself up, get over it. You’ll do better tomorrow.”
The biggest change may just be to be aware and present every time you make a decision about eating or drinking. Sometimes you may decide yes to the donut, and that’s fine! But if you take the time to think it through, you’ll likely make healthier choices more often, and you’ll probably feel better about your indulgent choices because you’re making them with the intention of thoroughly enjoying them.
Being mindful could mean making healthier choices, eating less, and enjoying our food more, so what’s not to love? It certainly seems easier than logging food and tracking calories, so start tonight! Notice everything about your evening meal: be wholly there for the preparation and consumption, and notice the sights and smells and sounds and flavors.
We’d love to hear how it went, so let us know in our community forums, on our Facebook page, or in Midlife & Menopause Solutions, our closed Facebook group.
If you ever get a weird tingling, crawling, numbness, or itching throughout your body, especially in extremities like hands, feet, arms, and legs, you might be surprised to learn that it could be related to menopause.
We all know the pins-and-needles feeling of realizing you’ve been in one position too long and your foot fell asleep, or of toes warming up after an afternoon of sledding. But when the burning or tingling all over your body happens for none of the usual reasons, it can be a little alarming.
Fear not. It’s called paresthesia, it’s not uncommon, and it usually stops when estrogen levels stabilize. Knowing that doesn’t make it any less annoying, so we’re going to talk about what it is and how to get rid of it for our Symptom of the Month.
What causes the tingling in my hands?
Menopause and nerves have a complicated relationship. Surprisingly, declining estrogen levels may be the culprit. Because estrogen levels affect our central nervous system, when those levels start to fluctuate, it can begin to affect our nerves.
The sensations can take a lot of forms: tingling, burning, crawling skin, cold, numbness, the classic pins-and-needles, and increased sensitivity. Women report symptoms from intermittent and mild to lasting and painful, even to the point of waking them from sleep.
What about in the face? Is that paresthesia as well?
This is most likely due to essentially the same cause, but with a different outcome. Most women report menopausal paresthesia of the hands, but it’s not uncommon to experience the same effects in the face. It can be particularly unpleasant, and can cause serious questions about your overall health. If your facial paresthesia is caused by the same declining estrogen levels, then the same treatments and remedies can theoretically be just as effective, which we’ll get to shortly.
Is the tingling sensation dangerous?
Paresthesia due to hormone fluctuation isn’t dangerous on its own, although numbness in the feet can cause women to lose their balance and fall when walking or running. Some women report the numbness or other sensation can make it temporarily difficult to grip or do fine finger movements.
When suffering a bout of paresthesia, it’s important to pay attention to how your body may be affected and adapt to any reduced ability. This can also lead to increased menopausal anxiety, so it’s important to pay close attention without stressing over it too much, or you’ll be doing more harm than good.
And of course, if you’re concerned about the severity of your symptoms, or if the tingling is disrupting your life, work, or hobbies, describe your symptoms to a doctor. If you can find a doctor who is particularly experienced with menopause symptoms and treatments, even better.
What can I do to help with these weird sensations?
As usual, there are lifestyle changes to try first:
- Eat well. A balanced diet with plenty of fresh fruits and veggies helps regulate the body and may help ease symptoms.
- Regular exercise improves blood flow and reduces tension, both of which can help relieve paresthesia. Stretch. Move.
- Get acupuncture and/or massage. Again, improving circulation can really help with paresthesia symptoms. Also, these treatments can be great for reducing stress, and stress often contributes to increased paresthesia symptoms.
- Sleep, hydrate, cut back on alcohol and caffeine. You know all these already, and should be doing them for all your menopause symptoms. Give your central nervous system all the support it needs to do its job well. Practice good sleep hygiene to maximize your down time.
- If you smoke, quit. Smoking is hard on circulation, restricting blood flow. Plus there are so many reasons to quit smoking at this time of life! If you want to quit but are struggling, talk with a Gennev clinician for tips on how to cut back and finally, quit entirely.
- Add supplements. B12 deficiency is a particular cause of paresthesia, and adding iron, magnesium supplements, and vitamins B, C, D, and E might help. If you suspect you may be low on B12, that’s a good time to see a health care professional.
When should I consult a doctor about paresthesia?
If none of these solutions make the paresthesia manageable, or if it’s impacting your sleep or quality of life, talk to a doctor about medical interventions like hormone replacement, topical creams, or a low-dose antidepressant medication for menopause symptom treatment. While paresthesia related to menopause is considered “chronic” (long lasting or recurring), there are ways to moderate the sensations until estrogen levels reach their new normal and sensations reduce or disappear.
Tingling and burning sensations can be caused by more dangerous conditions such as fibromyalgia or stroke, so if you have any of the following as well as the paresthesia, talk to your doc:
- Difficulty controlling arms, legs, hands, or feet; problems walking
- Increased urination or inability to control bladder or bowels
- Muscle weakness or paralysis
- Changes in vision or speech, slurring
- Fainting or black outs
- If the tingling is present in more than just an extremity, especially if it’s present in half of your body.
Paresthesia may not be pleasant and it might distract you when it strikes, but it generally isn’t considered painful. The more severe, sometimes more painful version is called dysesthesia and may be related to multiple sclerosis. If your tingling is painful, talk to a doctor right away.
We can help you understand paresthesia
- Meet with a Gennev Doctor – our board-certified gynecologists specialize in menopause and can help you understand your symptoms as they relate to hormonal shifts, prescribe a personalized treatment plan, and help you find additional support for paresthesia.
- Magnesium is so important for a range of bodily functions. It helps to reduce inflammation, relieve joint pain, muscle cramps, Restless Leg Syndrome, headaches, depression, fatigue, anxiety, and supports better sleep.
The information on the Gennev site is never meant to replace the care of a qualified medical professional. Hormonal shifts throughout menopause can prompt a lot of changes in your body, and simply assuming something is “just menopause” can leave you vulnerable to other possible conditions. Always consult with your physician or schedule an appointment with one of Gennev’s telemedicine doctors before beginning any new treatment or therapy.
We hear this all the time from women dealing with hormonal changes. Women tell us of creeping off to the bathroom at work when they feel a hot flash coming on, or driving to a distant drugstore to get something to relieve vaginal itch, or blaming their exhaustion on their kids rather than admitting to night sweats. It’s just too embarrassing to talk about, so we soldier on alone.
But we’re not alone. Like, really, REALLY not alone: By 2025, there will be 1.1 billion postmenopausal women in the world. One-point-one billion. That’s a massive potential support network, ladies, and that number doesn’t even include younger women and men who are eager to provide support if only someone asks. (hint hint)
Can we talk?
So, ask. Find your support system. Difficult times are always easier with your people in place, but menopause can be an especially important time for women to gather their tribe. Let’s take a look at all the stuff you may be dealing with, shall we?
- Empty nesting. “It’s like my house grew,” one woman told us. “Suddenly I had all this empty space. After years of griping at my kids about hogging the couch, all I wanted was someone to share it with.”
- Caring for elderly parents. Women are twice as likely as men to become the primary caregiver for an aging parent, usually while holding down a full-time job of their own. As one woman told us recently, “It’s just hard.”
- The emotional roller coaster. Many menopausal women report feeling anxious and depressed and having moods that swing more than a 1970s suburb. “My husband keeps trying to help, which is so great of him, but if he doesn’t stop it, there will be blood,” another woman admitted.
- Crappy sleep. Pardon our bluntness, but insomnia, night sweats, and increased anxiety can really shave off some of those critical zzzzzzzz’s, leaving us feeling irritable, exhausted, low on patience, and unable to concentrate.
- Low libido, painful sex. Reduced estrogen levels causes vaginal skin to thin and lose much of its natural lubrication, making sex painful. Because so many of us are reluctant to talk with our partners about what’s happening, there’s suddenly all kinds of friction (ha ha) interfering with our most important relationship.
- Dealing with symptoms at work. Our workplaces are havens of understanding, tolerance, and assistance, right? Well, ours is, but most are problematic for women dealing with hormonal changes. That woman desperately fanning herself with quarterly reports? Nothing to see there.
Seriously, gal, give yourself a break. There’s a reason superheroes team up to conquer evil, so be willing to send up the bat signal when you need help.
The benefits of support
Hot flashes, being caught off-guard by an unexpected period”these can be awkward moments, we agree”but too often women allow fear of embarrassment to isolate them. And that could be exactly the wrong thing to do for our emotional health. Plus, it perpetuates the THOROUGHLY OUTDATED IDEA that women should be embarrassed about their bodies.
A strong social network can act as a buffer between you and the more detrimental effects of depression and anxiety. Friends with wine and chocolate may not solve everything, but they can help. And sometimes a little boost on a bad day is all you need.
However, a mood boost isn’t all you get from your Partners in Perimenopause:
Information. This is a biggie. For example, did you know about vaginal atrophy? Yes, that’s a thing that happens, but using a specially formulated lubricant can delay or avoid it. Your friends probably didn’t know about it either or figured painful sex was just an unavoidable consequence of aging. How popular will you be if you help your best buds get their sex lives back?
Emotional support. Knock back the evil twins of depression and anxiety by talking through what’s happening. When we talk about what’s stressing us out, we react better and stay calmer, which can lead to clearer thinking.
Overall health benefits. Friends keep us from dying sooner. Yep. Having close friends may help us ward off that first heart attack. According to HealthDay, good friends are a helpful antidote to heart issues, diabetes, high blood pressure, and depression, and they can exert positive influence on us when it comes to lifestyle choices like exercise, nutrition, and smoking. One caveat: poorly chosen friends can make us sicker, so stick to your positive peeps.
Need a network?
While nothing beats an old-fashioned face-to-face complete with wine and brownies, online networks can provide satisfying social support. We’re building our community here at Gennev, so join us by joining the conversation: leave a comment on our blogs and engage with us on Twitter, Facebook, and Instagram. You can also find support via groups like the Red Hot Mamas. There’s no reason to go it alone. With quite literally millions of women to choose from, you can find that simpatico someone to make menopause healthier and easier!
Feeling alone in your menopause journey? Work with a Menopause Health Coach. Learn more.
If you’re gaining weight and considering doing a detox for your body, you might also want to consider doing one on your house. Hint: for once, it might not (just) be menopause that’s to blame.
Certain chemicals in your home, work, school, and other environments could be contributing to your weight gain. These chemicals, called obesogens, are endocrine disrupters, meaning they can interfere with hormones and may cause a range of health effects, including infertility and obesity.
Unfortunately, obesogens can be found in quite a few common household products, including, says the National Institutes of Health, “plastic bottles, metal food cans, detergents, flame retardants, food, toys, cosmetics, and pesticides.”
How do obesogens lead to obesity?
According to Dr. Patricia Salber, some obesogens can “disrupt the function of our hormones and others alter our gut biome, causing an imbalance of good and bad bacteria,” says Patricia Salber, MD, author of the blog The Doctor Weighs In.
(speaking of hormone disruption, read our piece on estrogen dominance with Integrative Women’s Health consultant Nicole Negron)
The end result? Research is still being done, but evidence points to slowed metabolism, lower available testosterone (which is a key fat-burner), difficulty utilizing stored fat for energy, increased fat deposition, and changing metabolic set points (your body’s ideal weight). Obesogens not only increase stored fat, they may then use that stored fat to attract and retain even more obesogens as well as other pollutant chemicals.
Even worse? You can pass it on to your kids.
How do I prevent contact with obesogens?
This is a tough one: the chemicals that are likely culprits are in a lot of common objects we interact with every day, which could mean the spring cleaning to end all spring cleanings.
Some suggestions for reducing obesogens in your daily life:
- Replace non-stick cookware with stainless steel or cast iron. (MightyNest is a good place to find safe cookware and bakeware.)
- Don’t buy objects containing phthalates. This is a biggie because phthalates are everywhere, including toys, soap, shampoo, water bottles, baby bottles, etc. Check the Environmental Working Group’s database to see how your choices rate.
- Avoid products containing bisphenol A (BPA) as usually in plastics like water bottles and food storage containers. If you have plastic food containers and just can’t give them up, just don’t heat food in them, which can release the problematic chemicals. Reheat your food in glass and invest in stainless steel water bottles.
- Avoid canned foods if they aren’t marked BPA-free. Yeah, we know. But BPA may promote fat-cell growth, so maybe soaking beans overnight isn’t quite such a terrible chore? To make life a little easier, NiftyHomestead.com has compiled a list of companies and their approach to BPAs in their canned goods.
- Dust often (obesogens can concentrate in household dust) and use natural cleaning products like vinegar and baking soda when possible.
- Ventilate well.
- Eat organic. Many herbicides, pesticides. and other agricultural chemicals contain obesogens.
(one great way to eat better is to shop the bulk aisle at your grocery store)
Protecting yourself and your family from environmental toxins might seem like an overwhelming, impossible task. But this isn’t one of those times when perfection RIGHT NOW is the goal as what’s important is to reduce, replace, improve every day and with every shopping decision. Change one thing at a time: get rid of your old non-stick skillet and buy a satisfyingly solid cast-iron one, for example. Immediately stop heating food in your plastic containers (or putting leftovers in them while the food is still hot), and as they age out, replace them with glass.
If you have information or a story to share on endocrine disruption, obesogens, or doing a detox on your home, we’d love to hear about it. Tell us your experience in the comments below, or on Gennev’s Facebook page or Midlife & Menopause Solutions, our closed Facebook group.
If her name looks familiar, it’s because Dr. Meagan Peeters-Gebler PT, DPT, CSCS, CMTPT, along with colleague Dr. Brianna Droessler-Aschliman PT, DPT, CMTPT, have been doing a monthly blog with Gennev for several years.
They’ve educated us on pelvic floor issues such as incontinence, prolapse, and sexual function; they’ve taught us about high heels and standing desks; helped us understand and relieve pain and keep our bones strong.
In this video/podcast, Dr. Meagan speaks with Gennev Health Coach Stasi Kasianchuk about pelvic function. What are the pelvic muscles? What do we use them for? How do we keep them strong and fit?
Watch the video of Pelvic health with Dr. Meagan Peeters-Gebler on YouTube. Full transcript is below.
The Path To Better Pelvic Health
Gennev:
Welcome to the Gennev podcast. In this series we talk with the experts about women’s lives and health in menopause. Our mission is to empower you with information that puts you in control of your health. We’re glad you’ve joined us. Let’s get started.
Coach Stasi Kasianchuk:
Today, like we talked about, I want to get your insight as a Doctor of Physical Therapy on pelvic health, pelvic stability. I’ll start off by introducing myself to our audience. So I’m Stasi Kasianchuk, I’m a Gennev menopause coach and I’m also a registered dietitian nutritionist with expertise in sports nutrition and exercise physiology. So with this topic I’ll start it off by saying I have a, I’ll call it somewhat understanding of pelvic health. I know it’s important from my anatomy and physiology classes and previous life as a group exercise instructor and personal trainer. I’m familiar with that musculature, but I know now that there’s been a lot more research and a lot more targeted approaches for pelvic health and stability. And so I’d love for you to just introduce yourself, your role as a Doctor of Physical Therapy, maybe give some insight into what that is in case some of our audience members are not sure of it. And then what is your role specifically in supporting women’s health?
Dr. Meagan Peeters-Gebler:
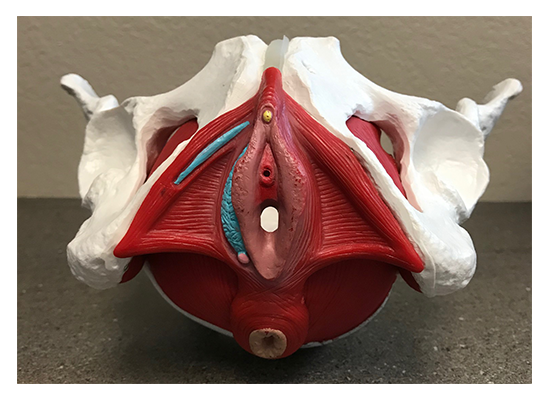
All right, thank you. My name is Meagan Peeters-Gebler and I am a Doctor of Physical Therapy as well as a postpartum and pregnancy corrective exercise specialist and a certified strength and conditioning specialist. So you know, as a Doctor of Physical Therapy, our introductory education is, is pretty general into the field of women’s health and pelvic health. So most of us who go on to pursue this specific area of study, it’s kind of postgraduate work and continuing education to acquire those skills and knowledge. And it is basically looking at the pelvis as a part of the whole, right. So you know, kind of as, as general PTs, we often look over the fact that it’s muscles, tendons, ligaments, nerves, bones. It is made up of exactly the same stuff that our necks and our backs and our shoulders are. And, and just making sure that we recognize its important role in the musculoskeletal system for pain, and like you alluded to for lumbopelvic stability but then also for continence or keeping, keeping our urine and stool in, and then sexuality. So I’m kind of putting all those pieces together and figuring out how mechanically as PTs we can promote better overall health and function to those, those areas.
Coach Stasi:
Excellent. That’s a great overview and gives us some good things to talk about and to dive deeper in. I would say so as an exercise physiologist and like I said, previous personal trainer and someone that also tries to make exercise a part of my life, in a way, honestly, my goals really are to stay healthy and to have longevity and understanding the learning more about the importance of musculature all over our body and pelvic health has really, as I’ve been in this field a little bit longer, learning more about that. So my general understanding is that the pelvic floor as you plays a role in obviously continence and making sure that urine and stool do stay where they’re supposed to be until we actually move them out on our own planning versus not. And then also from a core stabilization, I mean the pelvis is really close to the low back. It’s the connection to a lower body. So I’ve had an understanding that that strength in that area can also be important for decreasing risk of injury in other areas of the body. I would love for you to just dive into that. Correct me if I’m wrong on some things. And you know, let’s clarify some of this for our listeners.
Dr. Meagan:
Definitely. So I always like to point out that, you know, research has shown that disorders with continence and breathing actually have a higher correlation to low back pain then obesity or inactivity. So I think that is kind of a, a profound, you know, like way of, of really recognizing the importance of the pelvic floor, but then also the respiratory diaphragm as it relates to the pelvic floor in kind of a systemic container pressure management system. Right. We know that, that the pelvic floor, yes, is, is kind of a hammock of muscles that slings across the bottom of the pelvis.
Coach Stasi:
A visual!
Dr. Meagan:
Yeah. So it’s there, it attaches to, you know, the entire pelvis, it attaches to the tailbone and the sacrum. And it really does span and serve as like a structure and a structure to that the whole bottom opening of, of our body. And, and if there’s either weakness or incoordination, there is going to be an inherent vulnerability to everything that is stacked on top of that.
Coach Stasi:
Oh, that’s such a good point. Yeah. And is it possible? I guess what I notice a lot with a lot of the clients I work with through the HealthFix Program is that all of a sudden during menopause, things are just happening all over the place. And, they start to notice things that they may have not noticed before. So, you know, related to pelvic health, maybe all of a sudden there is more incontinence or they’re really wanting to improve sexual function or get their sexual function back. Is it possible, over time because someone may not be aware of this, we may not be working on supporting our pelvic health, then menopause hits with all these other things. And it’s accumulation of not supporting pelvic stability for years that happens at this point? Or is it really something that during menopause, the decrease in estrogen and what’s going on during menopause affects?
Dr. Meagan:
Yeah. You know, I almost so clinically I see it. Plus it’s like the straw that breaks the camel’s back, right: So, you know, gravity and bad habits and posture and life have been like cumulating insults on these poor structures. You know, we also know that the vast majority of women who are verbally taught Kegels are doing them wrong. So so it’s, it’s almost like, yes, we’ve been exposed to all of these challenges. If we’re even worse patients, you know, with without estrogen and without that good blood flow, suddenly these healthy, plump muscles get thin, and fragile and weak, and just the structural integrity automatically diminishes if you do nothing else besides ride it out. So, so wanting, wanting to either prepare before, be actively engaged during and, and figure out continued maintenance from a PT perspective I think is huge to navigate that time.
Coach Stasi:
Yeah, and I would say some of the questions that I get from a lot of the clients I work with, a lot of them are having back pain or knee pain. Are some things there. And I often recommend that they do exercises with a physical therapist, go to see a physical therapist to make sure that they’re doing exercises correctly. And you bring up a good point about the Kegels that most people are doing them wrong. So can you talk a little bit about what you see as maybe some challenges for women and then how you address that? And maybe give us some instructions on what is the correct way to do Kegels, if that’s possible over a podcast.
Dr. Meagan:
Right. Yeah, definitely. So you know, I think what, what we encounter typically in a clinic is that, kind of two diverging paths. One is that women are either squeezing with all their might, kind of everything between their ears and their eyebrows and their knees and their toes, like everything is gripping. And that is just too much that they end up actually generating too much pressure and making their pelvic floor have to work too hard.
And on the flip side, it’s that there’s absolutely no connection. You know, it’s like pelvic floor, what? Is that my anus, is that my, you know, like how do I even feel that, like I don’t feel anything moving. So it’s that women are either excessively connected or totally disconnected to those parts of the body. Usually what we do is we kind of take the approach of helping them find those body parts at the base of their pelvis through the breath. Because when we use the breath, what we can do is we end up tapping into some of the automatic reflexes and just exploiting the physics of how pressure moves through your body as a container to help them hone in on exactly what parts they should be feeling, in which direction, and to what extent.
Coach Stasi:
Oh, interesting. Is that something you could even direct me through right now over the over the podcast? I’ll give it a trial, like, you know what I’m feeling?
Dr. Meagan:
Yeah. So, so kind of the spiel that I like to give is that our body is a container, right? We have air on top in our lungs and in our rib cage. Then we have a diaphragm that separates our air from our guts, then we have our guts. And then we have our pelvic floor, right? And as air moves through our container, the shape of our container should change. And the pressures inside should also change. So as you inhale and you inflate your container, your rib cage should expand in all directions to accommodate that, that added air. Your diaphragm should drop to make more space for air. And in doing so, your guts should bulge out to the front and down to the bottom a little.
So on an inhale you should feel your perineum, your pelvic floor, kind of that space between the vaginal opening and the rectum and the anus drop slightly in response to the fact that air has been added to the system. Okay. On the flip side, when you go to let the air out and exhale, which you’re going to feel is your rib cage shrinks, your diaphragm actually lifts up kind of following the air out of your body. That creates a loop, a little vacuum that pulls your guts up and in as well as your pelvic floor. So we like to get gals kind of rocking and rolling with that breathing rhythm where on the inhale inflate, notice the pressure in the expansion. And then on the exhale, think about gently lifting two beans, right? So think about squeezing around and pulling up and in at the vaginal opening as well as at the anus.
And you want to include, well the front and the back openings because the pelvic floor muscles sling around both of them. Yes. Okay. So you inhale, inflate, feel things descend and then you exhale, lift, gently squeeze and notice that there’s a lifting action that happens.
Coach Stasi:
Wow, that’s incredible. I don’t, I think I’ve ever thought that process through and it’s a good reminder of really that deep belly breath versus the short inhalations that we… myself, I’ll speak for myself to have a tendency to do more often where that is such a valuable benefit. And I actually, I have never heard of that comparison before, so that was really helpful to take that time to really think about where is my pelvic floor, where are those muscles and what are they doing?
Dr. Meagan:
Yeah. Yeah. I tend to also see a lot in the clinic where women have become what we call paradoxical or exactly the opposite because in their brains they want to lift up when they’re inhaling, because they want in in in all to go together, and in doing so they actually manipulate both the diaphragm and the pelvic floor to be coordinated exactly opposite of what we want and it’s this constant then tug of war and the pelvic floor just kind of freaks out and quits either by shutting off and allowing leaks or by spasming and tightening up to try to prevent them. That dysfunction kind of shows up.
Coach Stasi:
Oh, interesting. Yeah, so kind of the extremes that we had for our overachievers out there that they have been doing too much or too hard for for years over time.
Gennev:
You can now manage your menopause with Gennev. We’ve helped thousands of women take control of their health with our team of doctors, coaches and products. Join our membership program called HealthFix and work with one of our menopause coaches on your personalized menopause plan. Learn more at Gennev.com.
Coach Stasi:
Well, and it sounds like there’s opportunities for both sides. There’s prevention. So if women are in perimenopause or even pre-menopause, which I’ll admit, I’m pre-menopause, I’m 36 years old, still menstruating regularly, but it’s, so much of this is important for preparing. So I’m thinking a lot about, I know probably in the next 10 years there’s going to be some changes. And so would you say that doing these types of exercises, being aware of the pelvic floor, even before menopause, or definitely in peri-menopause is beneficial for women’s health?
Dr. Meagan:
Definitely. You know, I think across the whole lifespan, you know, I think, I think this is one of those muscle groups that we just kind of take for granted. You know, until there’s a problem with it, it’s off our radar, you know, and I think there’s a little bit of attention postpartum and then it’s like, unless again, unless it’s causing a major problem, we, it just loses focus. But you know, it’s a muscle. It’s a muscle group, use it or lose it. Right?
So I think by having a, a mindful focused approach on including the pelvic floor in your regular exercise routine, you can definitely help counteract some of the loss of muscle health and function from that reduction in estrogen. So I usually try to get women to the point of you know, if you’re, if you’re following a good exercise program and doing a mix of, you know, strengthening and conditioning if you are breathing correctly, correctly and including your pelvic floor during the task that you’re doing, those count as your daily pelvic floor exercises. You know, not everyone necessarily has to sit and do three minutes of Kegels, driving Kegles, uou know, all of the things that often time, you know, we are led to believe is necessary.
But if you can weave it into your day, all the better. And then you’re also gaining the functional benefit of, of your body learning and knowing how to use your pelvic floor to give you stability when you pick up your grandchild or push the door open or all of those things.
Coach Stasi:
That’s great. That’s great to know. It’s great to know that it doesn’t have to be a separate thing. Cause a lot of the women I work with, it’s, they’re already dealing with a lot. And so adding one more thing, like now you have to do Kegel exercises, even if it is just three minutes can really be another straw that breaks the camel’s back. So that’s helpful to know that recommending just breathing appropriately, which has, benefits in so many other areas too, can help them to target that and just bringing mindfulness and focus to that.
Dr. Meagan:
Yeah, no, don’t get me wrong. You know, if you’re in pelvic PT, you’ll be, you’ll be spending some time doing those specific exercises. But like I said, I like to get gals to that point where it’s just integrated in your day because then it actually happens, then it’s not something you have to remember to do.
Coach Stasi:
Yeah, exactly. Well, let’s talk about that. That’s a great point as well. And this is helpful for me, but if someone is that our listeners are listening to this, maybe thinking, Hmm, should I see a physical therapist for this or should, can I just focus on breathing and be, okay? Where’s the line where it’s like, you know what, having someone that’s watching you, giving you instruction where you have an appointment that you’re going to and potentially could provide additional therapy where, where’s the line? Or how did, how do women decide that?
Dr. Meagan:
So that’s a little tricky, right? I’m a pelvic PT, so I think everyone should come see a pelvic PT. I think that, you know, knowing that so many women are, or doing something just so subtly wrong that can really make or break their success that, you know, even just a single consultation with a pelvic PT can be so tremendously valuable to make sure that you aren’t making matters worse.
You know, I, I see women every single day where there, you know, maybe doing a sneaky breath hold in their Kegel and then they wonder why they are still leaking, when they even tried to do a Kegel you know, as they sneeze, it’s like, well you’re actually holding your breath, which is pushing down and your pelvic floor can’t combat the forces there. So so I think having another set of eyes to give that feedback is, is just, you know, priceless.
You know, public PTs are gaining accessibility. For a long time, you know, we were kind of far and few between, but I do feel like you know, there are some, some good resources out there for people to find pelvic PTs. You know, like our national organization, the American Physical Therapy Association has a website. Like find a PT: you can put in “women’s health and pelvic PT,” put in your zip code or city and it can help you locate someone who has good training and resources as close as possible.
Coach Stasi:
Oh excellent. Thank you for that resource. Cause I think that’s helpful with us working with women all over the country. How they know, okay, you know, if I’m looking for a physical therapist that specializes in this, how do I find them? And that’s also a great point: Knowing to ask it, it sounds like they shouldn’t just go to any PT clinic and say I need physical therapy. They should be saying, I want to work with a physical therapist that has expertise in pelvic health. Is that correct?
Dr. Meagan:
Yes. Yeah. Yeah. you know, we do get exposure in our professional training, but like I mentioned, the vast majority is in kind of that postgraduate, continuing education work.
Coach Stasi:
And can you talk a little bit about that? What makes, what have you done to become an expert in this area? What that additional training looks like? So, you know, it helps our listeners to understand and also to make sure that they aren’t going to someone that perhaps doesn’t have that expertise and potentially do more harm.
Dr. Meagan:
Yeah. So there are, there are various groups that offer continuing education. Most of them provide two to three day courses on the weekend where PTs will attend. And it is learning both the kind of didactic information and in depth learning of anatomy, physiology, what’s normal, what’s abnormal, what’s common and what’s uncommon. That combined with extensive lab practice where these physical therapists are practicing on each other. You know, so we’re learning as a patient, someone is doing these exams or these techniques on another PT so that you, you have that experience and that kind of level of understanding to know what, what the person on the table is also going through as you’re providing the services. You know, and, and typically it is then a sequence of courses that most people will end up going through depending upon their interests. You know, if they have more interest in bowel function or dysfunction, pregnancy, postpartum care, pelvic health but, and even in the introductory classes the therapists are going to be exposed to treating urinary incontinence, bowel incontinence, pelvic pain, painful intercourse. All of the things that we, we tend to see women in the clinic for.
Coach Stasi:
Okay. Yeah. So, and, and it sounds like there might be specific approaches for each of those things. So it’s not just a blanket approach for pelvic health. It’s what is your specific concern and here’s the approach for you.
Dr. Meagan
Definitely. Definitely. Yeah. Yeah, yeah. I was going to circle back to what you were saying about knowing if you need a pelvic PT within the last question. And as I was listing those things off, I think that’s, that’s kind of a nice, nice, way to put it on the radar is if you’re leaking anything, out of your vagina or your anus, involuntarily, that’s not normal. And that’s not okay. You know, it may be common and it may be brushed off because of, you know, whatever reason your mom or grandma may have told you. But absolutely there are things that can be done about it that are conservative and quite effective. If you’re having any pain, painful gynecological exams, painful wiping you know, with bowel movements or after urinating, any kind of painful vaginal penetration for intercourse. That should not hurt. And those are also indications that finding a PT you know, as well as working with your, your medical, other medical providers, but definitely things that, that pelvic PTs treat, I think are good to have, good to have on the radar and seek, seek more help.
Coach Stasi:
Yeah, absolutely. And I appreciate you listening out those symptoms because you make a good point. A lot of times, and I see this in a lot our, our Facebook group and when women are talking with each other, they have great community support, but sometimes when everyone in the community is experiencing pain and incontinence, they normalize it. And while it may be, I don’t, I don’t want to say no, I hesitate to use the term normal, maybe common, like you said, during this time of life. And, but it does attention and it doesn’t have to be the normal. It shouldn’t and it isn’t normal. And really does deserve treatment and there’s treatments out there and there’s no shame in it. You know, I think that’s the other part. Sometimes women when I’m talking with them may feel a little hesitant to talk about things that are going on in that area. But it’s important to know that’s a really important part of health and not to feel shame and to know that they can get support.
Dr. Meagan:
Most definitely. Yeah. Yeah. Most of the women that I end up seeing and talking to in the clinic tell me, Oh my gosh, I wish I would’ve known this five, 10, 20 years ago. You know, it’s, it’s again, I think it’s gaining you know, its ability to be talked about more comfortably and knowledge is power. But yeah, you’re right. It still is something that for some reason women are felt to, to feel, you know, some, some personal level of shame about, but should not.
Coach Stasi:
No. And that’s where we’re hoping here at Gennev to kind of change that perception of menopause, this time of life, and really provide the resources that are out there. And based on what you said, it sounds like most women, if not all, should have a pelvic floor PT on their healthcare team or on their menopause support team during this time in their life. I mean, it’s putting the tool in the toolbox to really help them thrive.
Dr. Meagan:
Yes, most definitely.
Coach Stasi:
Excellent. Well, I really appreciate your time today. Is there anything else that you want to add or last tips or points? And give your clinic information and location for any listeners that may be near you just to finish up with.
Dr. Meagan:
Yeah, I mean, I think you know, thank you for having me. I think it’s just awesome that we’re getting the word out and, you know, like I said, knowledge is power and, and knowing that there’s hope and that it doesn’t mean that you have jump on a medication. It doesn’t mean you have to jump to surgery. You know, and there there’s always the potential to make these even slight improvements and, and it’s not, it’s not terribly hard work to do once, once you get committed to it. It’s just a lot of, a lot of changing and bringing things to awareness that can have pretty profound positive impacts on people’s lives.
I practice out of Orthopedic and Spine Therapy. We are a private practice in Wisconsin in the Appleton, Wisconsin area and we have clinics kind of scattered throughout the state but pretty much focused in the Fox Valley area.
Coach Stasi:
Okay, excellent. Well good information for our listeners to locate you or certainly you gave them the information and that was the what was the, the organization is the, the American Physical Therapy Association?
Dr. Meagan:
Yup. APTA.
Here’s to better pelvic health and wellness
Coach Stasi:
Okay, excellent. And you can go on there, put in your zip code and then specifically look up women’s health and pelvic health to find someone that is trained in that.
All right, well just to finish up on my end, I do want to put a plug out there for our HealthFix program. I am a menopause coach as I mentioned in the beginning working with that program. And having that membership, it’s a subscription based membership, you get the opportunity to work with someone like myself and talk with them out through calls as well as have supported accountability between those calls. And so it can be an opportunity as well if you’re thinking, I don’t know if I should go see a pelvic PT even though I think after this we all should, but if you have questions about that or just questions about any symptoms you’re experiencing during menopause, signing up for the HealthFix program gives you the opportunity to have some of those questions answered, provide resources, information and support around finding what the next steps are. Perhaps it’s finding that physical therapist in your area or perhaps it’s just figuring out what that next step is for you, whether it be pelvic health or other menopause symptoms. So sign up for that HealthFix program and I hope to be working with more of you that are listening to this podcast today. So thanks very much Meagan, and I hope you have a great rest of your day and I’m sure we’ll collaborate again soon.
Dr. Meagan:
Wonderful. I look forward to it.
Coach Stasi:
All right, take care.
Dr. Meagan:
Thank you.
Gennev:
Thank you. Thank you for listening to this episode of the Gennev podcast. Remember, you can subscribe on iTunes, Google play, Spotify, and just about anywhere you get your podcasts. Gennev is your online destination for menopause, doctors, coaches, products, and education. You can find us at Gennev.com. Thanks for joining.
Learn more from Coach Stasi Kasianchuk and Dr. Meagan Peeters-Gebler by searching on their names on this site.
If you have issues with your pelvic floor or have improved your pelvic health, we’d love for you to talk with us about it. Please join us on the Gennev Community forums!
According to research by Strava, most of us have caved on our New Year’s resolutions by (wait for it)”¦ January 12.
To which we say, “shrug.”
We’re not huge fans of NY resolutions around here, preferring instead to help women achieve their best health all year long. But if you want to get back on track, or if you’re struggling to stay resolved, our awesome DPTs (Doctors of Physical Therapy) have some tips that might help you in your efforts.
Here’s what we learned from Dr. Meagan Peeters-Gebler of Orthopedic & Spine Therapy and Dr. Brianna Droessler-Aschliman from Missoula Bone & Joint about staying motivated and safe when you start or ramp up your better-health routine.
Why do we quit to revitalize our life fitness and how can we carry on?
Our reasons for not sticking with our health goals are probably as varied as we are, but Bri and Meagan do note some trends. Since forewarned is forearmed”¦
One: Unexpected results like muscle soreness, fatigue, pain
We all know exercise can hurt, but what we may not expect is how much it can ache and how long the hurt can last. If you go all-out on January 2, you may be surprised how lousy you feel on January 4.
Solution: Bri suggests you work with a coach, PT, or trainer at your gym to ramp up your efforts slowly and appropriately. Know and be honest with yourself as if hurting is likely to make you quit, create a plan that will minimize the ache. Even a small improvement to your fitness is vastly better than none at all.
Are you experiencing joint pain or arthritis and not sure what to do? Check out our blog with Orthopaedic Surgeon Dr. Darcy Foral.
Two: Poor training
A couple weeks in, poor training is biting us in the backside. At about this mark, says Meagan, if we’ve been doing a daily challenge like an ab workout, the repetitive motion and any poor form is really starting to show up as back pain or another overuse injury.
Solution: Daily challenges don’t take into account our bodies’ needs for rest and varied motion. Anything that has you doing the same pattern of movement day after day is probably not a great idea. Meagan says you can make it safer by (a) checking your form with a health/fitness professional, (b) mixing it up so you’re not doing the same movements every day as maybe alternate with an exercise that targets another part of your body, and (c) taking rest days.
A month of squats can be really hard on your knees and pelvic floor; squats done properly and mixed in with cycling, swimming, walking, and rest can be really beneficial.
Three: Inexperience
Either we push too hard and hurt ourselves, or we don’t know our body well enough to judge if a pain is normal and OK, so we quit to be on the safe side. Gyms fill up in early January, Bri tells us; physical therapy appointment slots fill up the rest of the month.
Solution: First a caveat: Every body is different, so these are just general guidelines to consider. If you’re hurting and you’re concerned about it, by all means, see a doc or PT for a diagnosis and recovery plan.
According to Meagan, if a pain is so localized that you can trigger it by pushing your finger on a certain spot, and The Spot comes back every time you do an activity, that’s a big red flag. Stop doing the thing that hurts and give your body time to recover or see a doc. If the ache moves around or comes and goes or can be covered by your palm (as opposed to a finger), it’s less likely to be urgent or acute.
Bri adds, sharp pains or pains that cause you to compensate by shifting your form are definitely signs your body wants you to stop. If your Achilles tendon hurts and you start favoring that side, you could set off an unhealthy chain reaction where now your knee hurts, your hip hurts, your IT bands ache, your lower back is sore”¦ you see where we’re going with this. Stop. See a doc. Rest.
One way to know if your form or gait is off is to check in with a work out or running partner, Meagan says. Anyone who’s exercised with a buddy knows you start to recognize your partner’s “natural” form, often without being consciously aware of it. If your gym friend or running buddy asks if you’re hurt or limping or otherwise doing something funny, listen. They may be picking up on cues you’re missing. And if it’s obvious to the non-professional, you really need to pay attention.
If pain starts with the activity and intensifies as you continue, and if it hurts worse at the end than at the start, that’s a clue that tomorrow is a rest day. Pain that is with you at the start and lessens or goes away completely is probably OK to power through, as long as it’s not severe, localized, or changing your form.
Four: unrealistic expectations
Pair crazy expectations with someone who’s just starting to get to know their body’s abilities and limits, and you can be in for some disappointment. As Bri tells us from her experience with clients, your body may hurt more or your performance may improve more slowly than you expected, or you may be plateauing in terms of weight management. Any or all of these can cause us to throw up our hands and head back to the couch.
Solution: It’s OK to re-evaluate your goals, says Meagan. If you decided to run a marathon in 2019, maybe reassess and see if a half-marathon or sprint triathlon is easier to stick with. That’s not to say you couldn’t run a marathon in 2019, just that the lesser pressure of a different goal might make it easier to stay motivated. When we set resolutions, we can get compulsive about staying on track. Allowing yourself permission to reassess may be the difference between healthy achievement of that new goal and “failure” and/or injury with the old.
Blame social media for some of this tendency to be unrealistic, Bri says. Your friend’s Facebook posts about getting fit may make it look like she went from unhealthy to Olympic while hardly breaking a sweat, but you may not be seeing the steps between. In addition, your body is uniquely, wonderfully yours, and your fitness journey will be too. Applaud your friend’s achievements, but don’t compare them with your own.
Five: underestimating the process
There’s a tendency among those new to fitness to believe that it’s a constant, steady progression, and each day you’ll be better than the previous day. That’s just not true, but that myth is often why it can be hard for some new athletes to take rest days.
Solution: If you’re new to the fitness thing or just adding a new activity, talk with someone who’s been doing it a while. Ask them about their experience so you get a better idea of what’s involved. We do this for new employees when we “onboard” them, right? No one expects you to know everything your first day at work. Have equal patience with yourself your first day at a new activity. Also, having a buddy to check in with and stay accountable to is a great way to stay motivated.
And rest. “You’ll be a better, stronger, faster athlete and able to perform longer, if you recover between workouts,” Meagan says. “There’s a reason your fitness watch or app has built-in recovery periods of 24 hours or 12 hours or whatever,” Bri says. “Follow it.”
Be patient and understand that bodies are bodies and you’ll have good days and bad days. Don’t let a belief that every workout should be better than the one before be a reason that you quit or push yourself to the point of injury.
This is particularly important for women in midlife. Your body may not respond to changes as quickly or dramatically as it did when you were younger, and energy levels during the perimenopause/menopause years can be really low. Hormone fluctuations, fatigue, interrupted sleep, greater stress can all make exercise really tough. However, most women find that this is temporary (though “temporary” can mean months or years), and it gets easier when hormones level out on the other side.
Six: too few rewards for the effort
The numbers on the scale aren’t moving the right direction. The tape measure isn’t showing the anticipated improvement. Your clothes fit the same, no one’s mentioned your change or glow or new found energy. So what’s the point of all this work?
Solution: redefine “rewards.” First, understand that while change may not be happening on the outside, it almost certainly is happening on the inside. Muscles are getting stronger, your heart is getting healthier, maybe blood sugar levels are evening out, your lungs and brain and endurance and immune system are all seeing benefits. The change may be incremental, so small and slow you don’t notice, but suddenly you’re not out of breath from taking the stairs or you’re sleeping a bit better. Appreciate that even if you can’t yet do more reps or lift heavier weights or go to a smaller size pair of jeans
And reward yourself. As Meagan says, celebrate your accomplishments. You’ve made it a month! Buy yourself a new pair of really good socks or a better sports bra or a new swimsuit. Post a note on your mirror congratulating yourself for sticking with it this long.
If you’ve dropped your new fitness routine, no worries. You didn’t “fail.” “Respecting your body isn’t failing or quitting or being lazy,” says Bri. “You took a few days off to rest and re-evaluate, and now you’re ready to start again.”
As Meagan says, the real achievement is in balancing your approach so you can continue staying active for the long term. Staying realistic, seeking help when you need it, and resting when rest is called for can all help you get past January 12 (or Valentine’s Day or spring break or swimsuit season) and on the path to life-long fitness.
How are you doing with your resolutions or your general fitness goals? We’d love to hear your story and solutions, so please share with us by commenting here, or joining the conversation in our community forums. You can also reach out to us on Gennev’s public Facebook page or in our closed Facebook group.
Hey, SuperGal, before you head out on that bike ride or hike or claim your spot in spin class, have you done what you need to do to protect your body?
Yes, exercise is great for you as for your heart and lungs, your stress levels, your bones, your brain, ALL THE THINGS as but friction, moisture, and pressure in the wrong time, place, and amount can all derail your efforts to be healthier.
To learn more about what bugs us when we’re trying to get fit, we talked to our genius PTs, Meagan and Brianna.
The problem with friction
When skin rubs on skin or skin rubs on something that doesn’t slide very well, you can end up with some nasty chafing. Ask any athlete who whips off her sports bra and leaps into the shower, only to find when the water hits her that her bra has been rubbing her raw for the past couple of hours. There’s usually some shouting.
Friction not only hurts, it can leave us vulnerable to infection, so let’s talk about how to avoid it.
Gone are the days of cotton tees and sweat pants for exercise. Love it or hate it, our PTs tell us, Spandex and other slide-y fabrics are much better choices.
If you’re a biker, Meagan says, invest in a good pair of bike shorts that grip tightly around your thighs, yet move with you. These slide easily over your bike seat, which reduces friction. This is especially important if you’re generating a lot of sweat and spending a lot of time in the saddle.
Chamois (pronounced “sham-ee”) creams and lotions also reduce the skin-on-skin and skin-on-fabric resistance. Apply liberally, Meagan says, on the outside of any parts that get involved, including the external girl bits like the labia minora and majora. Also get the inside of the thighs, any creases or folds in the skin, anywhere your clothes rub repeatedly. “Everything needs to have the ability to slide and glide on itself rather than create friction and hot spots,” says Meagan. Oh, and do not wear underwear under your bike shorts as that nullifies the benefit.
Hint: if it burns when you urinate after exercise, you probably need more help with friction. “The acidity of urine flowing over the skin “in the neighborhood’ causes that pain and burning and indicates points of chafing or friction. This is potentially a risk for infection, so note the spots that burn for chamois cream next time.”
According to Bri, clothing choices aren’t just for bikers. Runners, walkers, and hikers may find that compression shorts reduce unwanted friction. You can wear your Spandex under other clothing, if you don’t feel comfortable with the skin-tight look.
Runners can tell you about the wonders of Body Glide and other friction aids: these usually come in a stick like deodorant and can be rubbed on all the spots where you normally chafe, like under bras, between thighs, around toes, and on the bottoms of your feet. They last a long time (which is why many athletes prefer it to Vaseline) and can be reapplied as necessary.
Pressure and exercise
Friction isn’t the only cause of discomfort; pressure in the wrong places can be painful and lead to more serious damage.
What’s the problem with pressure? Compression in the wrong spot during exercise can reduce proper blood flow, Bri says. If your toes go numb during running or biking, that’s a good indicator that there’s pressure somewhere that shouldn’t be.
And pressure doesn’t just affect a single area. Discomfort from pressure may make you change your posture as you exercise, and getting out of proper alignment can set off a chain of painful issues.
“Pressure is another reason to invest in a good pair of bike shorts,” Meagan tells us. “They come with what’s called a chamois, which is like a big pad sewn into the crotch. It provides a cushion and absorbs friction. You want your saddle to be hard and rigid to support your pelvis, but that can be hard on the bony spots.” With a chamois built in, the bike shorts provide the cushion so the seat doesn’t have to.
Also, Meagan says, be sure your saddle fits you right. It should fit the shape of your pelvis so you’re taking the pressure on your “sit bones.” Those really big, thickly cushioned seats might look comfy for your tush, but in fact, they can make things worse by allowing too much sliding around. Not only does that cause more friction, it also reduces your efficiency as a cyclist.
Another way to fix pressure problems is to make sure your bike is fitted correctly. A good bike shop can make adjustments so your seat is the right height, the handlebars are in the correct position, the length of the bike is good for you, etc. This can make you a more efficient and powerful biker, but even more, it can help you be more comfortable and avoid pressure problems.
You want your bike seat to be level or 2 as 3° “nose down,” Meagan tells us. If it’s tilted too far forward, you’ll slide down and off, and your arms will be doing too much work to keep you in place. If it’s tilted too far back, you’ll be putting a ton of pressure on your pelvic floor muscles and tail bone, and that’s not where you want it.
The shape of your saddle should fit your “sit bones” so you’re resting on your skeleton, not counting on the hammock of pelvic floor muscles. If you sit on a hard chair, you can feel the bones you want to use, Bri says; move around until the pressure is in the right place.
Your insurance may even pay for you to get your bike professionally fitted by a physical therapist, which both of our PTs vigorously recommend. “It’s a good, proactive measure,” Bri says. “Especially if you’re going on long rides or you’re bike commuting more than a couple of times a week.”
What are you avoiding? Spending too much time on a bike that doesn’t fit can cause neck and shoulder pain, headaches, numbness in your hands from taking too much of the pressure there, numbness in your feet, tailbone or lower back pain, knee pain, possibly even carpal tunnel syndrome (PS get bike gloves if this is a risk factor for you). Some women even complain about numbness in their intimate areas.
And, Meagan adds, if you have surgery or take time off, or if you’re ramping up your training, consider that a cue to check your bike fit, especially if it’s been a couple of years.
Incidentally, everything we’re telling you here also applies to spin class. Just because your bike isn’t going anywhere doesn’t mean you’re off the hook for pressure, friction, etc. Bri suggests you spend time getting a spin bike to fit you perfectly, then record all the relevant numbers and measurements for next time.
Pressure as from the inside
Another thing you really want to beware of is any pressure that’s coming from the inside that shouldn’t.
Says Brianna, “If you’re experiencing heaviness in the pelvic floor or chafing at the vaginal opening, that can be a warning of early prolapse at the anterior or posterior vaginal wall. You should stop the exercise and get to a doctor or physical therapist to get equipped with a pessary or another device to support the vaginal wall and prevent chafing.”
For runners, Meagan says, “If you feel like your tampon might fall out while you’re running, that can be a clue that there’s a prolapse happening, so you want to get that checked out. Also, a menstrual cup can help with internal pelvic health during activity. They’re made of silicone or other rigid materials that slide and glide rather than absorb and cling and create friction like a tampon.”
Moisture as not always a good thing
“Moist” is no one’s favorite word, and there’s a reason for that: a lot of the time, it’s not doing your body any favors. Bacteria loves a good moist place to hang out and cause trouble, so it’s best not to give it the opportunity.
When it comes to exercise, wicking fabrics are the bomb. They may be more expensive, but it’s worth investing in a few good pieces, Bri says. Get a couple of good sports bras, shorts, shirts, socks. If you treat them right, they’ll last a long time and save you a lot of annoyance.
And finally, while you may want to spend all day in your bike shorts (HA!), resist the temptation. Sweaty moisture isn’t great for your private areas.
“Practice good hygiene after exercise,” Bri advises. “Don’t sit in your exercise clothes. Get a shower if you can, but at least wash with warm water, no soap, no scrubbing. If you’re really pressed for time, find some wipes that are OK for that area that can cleanse sweat and get rid of bacteria.”
Let’s face it, 50 isn’t what it used to be (and that’s a good thing). Many of us are staying physically active well into our middle years and beyond. To keep enjoying exercise, be sure you’re protecting your body from little irritations that can turn into bigger problems.
How do you protect your body during exercise? Have you gotten good (or terrible) advice you’d like to share with the class? Please feel free to share with the community by leaving us a comment below, or talking to us on our Facebook page or in Midlife & Menopause Solutions, our closed Facebook group.
Health Coaches are a vital link in connecting women with the care they need to take control of their menopause. Gennev Women’s Health Coaches are Registered Dietitian Nutritionists (RDNs) who, in addition to their extensive nutrition training and experience, have been trained specifically in supporting women during menopause. They provide support, recommendations, resources, and accountability to help you navigate menopause and thrive along the way.
We sat down with Gennev’s Director of Health Coaching and Dietitian, Stasi Kasianchuk to gain an insider’s perspective on being a health coach, and how they offer much needed support to women in managing their menopause.
How did you get started in health coaching?
Through my own interests and enjoyment in nutrition and exercise I have come to learn how this can help me feel my best and wanted to share this with others. Through continued education and training as a dietitian in behavior change science I have learned approaches that I use to support my clients in finding the habits and practices that are accessible and realistic for them to implement to feel their best. Throughout my career I have come to learn more about other aspects of our lifestyle, in addition to exercise and nutrition, that impact our quality of life such as sleep and stress management. Integrating these things all together I can support women holistically.
What do you find most rewarding in your work?
Working with and supporting amazing women who, no matter how bad their menopause symptoms, are showing up to learn, willing to be vulnerable, and embrace their beautiful, changing bodies. This is by no means easy. In a society that does not value age, especially in women, it can be hard and uncomfortable to have conversations about menopause. However, we need to have these conversations to support future generations of women. My clients are a part of this change and I love being part of this movement. There is work to be done and the future is bright.
Why should someone consider working with a health coach?
Our health coaches are dietitians who use a supportive and compassionate approach personalized to our client’s needs. Menopause can create uncertainty and isolation. Working with a Gennev coach you have a knowledgeable expert that can answer questions to mitigate uncertainty and provide support. Most importantly, we will always remind you that you are not alone and menopause isn’t forever.
What advice can you offer for someone preparing for their first session?
Calls with your coach are opportunities for you to share your story. It can be scary at first, but know that there is no “wrong way” to do it. It can be helpful to have your main questions, concerns, and primary symptoms causing disruption to your life written down to refer to. If you have questions about supplements have these near you, so you can answer questions about brand, dose, and ingredients.
Are there any themes you have seen recently in your work with Gennev members?
Focusing on more pleasure, joy, and fun has been a theme with several clients recently. While this may differ from what they found pleasure in five or ten years ago, I find that women really benefit from exploring this to learn what joy is for them now. Once they do, and start implementing these things more often, there is a certain freedom and liberation that can occur. When we center on joy in our lives, menopause symptoms aren’t quite as all-encompassing anymore.
What is your personal message to women about the menopause experience?
For too long menopause has been disregarded and women have suffered in silence. This needs to change. We have an opportunity to reclaim this time of life for women to be one of celebration and opportunity rather than doom and gloom. That’s not to say that every day will be bliss and when it’s not, pretend it is. Instead, it’s an invitation to start the conversation, acknowledge the discomfort, and be open to exploring the possibility that there is more celebrating to do.
Schedule a Health Coach Consultation to create your personal plan to take control of your menopause.
About Stasi Kasianchuk
As a sports dietitian and exercise physiologist Stasi approaches her work with her clients through the lens of optimizing performance by supporting and working with an individual’s physiology. Having worked with a variety of clients over the past decade including collegiate and elite athletes to now working with peri/post-menopausal women, she has come to realize that everyone wants to optimize their performance in life. Recognizing that this often looks different for each individual, Stasi uses a personalized approach to help women feel their best. Outside of work Stasi enjoys trail running, swimming, weightlifting, yoga, group exercise classes, and biking; weekly trips to her local farmers market; cooking at home and dining out with her partner; and walks with her dog, Plinko.