you know there and you are here. And at the same time
While the world has woken up to the menopause conversation, most of that conversation revolves around defining the problem. And when it comes to the workplace, the problems are real. The Mayo Clinic recently published a study showing menopause symptoms cause an estimated $1.8 billion in lost work time per year in the U.S., and $26.6 billion when medical expenses are added.
For women experiencing menopause, unsupportive working environments can lead to major career interruptions. One survey found nearly 20 percent of women in menopause have quit or considered leaving a job because of their symptoms.
In the UK “ despite the government stopping short of introducing legislation to protect the rights of women in menopause “ employers are enacting workplace policies.
The groundswell is growing, and US employers will also be under the menopause microscope as this conversation continues. While there are many ways an employer can support employees in menopause (including adding Gennev as a benefit), a clear policy is an ideal place to start. We brought together a team of HR professionals, medical experts who specialize in menopause, and seasoned executives to give employers a starting point.
When addressing menopause, there are several places to begin. In this guide, we’ll discuss how to consider women in menopause in all your conversations; how to integrate menopause into your existing benefits ecosystem and/or add new benefits and policies; physical improvements you can make in your facilities; and how to start a conversation that goes beyond the HR team.
Integrating Menopause Into Your Existing Benefits Ecosystem
Step one: Consider her
In many companies, we don’t create menopause benefits because we aren’t thinking about women in menopause. Creating a mid-life female persona can help with that. Here’s a sample persona:
- Mona, a Senior VP in her late 40’s, is experiencing the early stages of menopause, also known as perimenopause. Imagine, for a moment, what it feels like for Mona to show up for work and lead her team through a tough week when she is truly exhausted from not sleeping. Or to experience a hot flash in the middle of a presentation that she is presenting to the CEO. Or how the indignities of mood swings can create challenges for how she interacts with her team. All this, and Mona’s eyesight is becoming blurry as well. Mona feels motivated as ever, yet burdened by the challenges thrust upon her by menopause.
When we present this persona for open-enrollment scenarios, we gain insights into how she navigates through the benefits ecosystem that already exists to support a menopause journey. Her uses may include:
- Reimbursement of menopause products through Lifestyle accounts. Mona can be reimbursed for cooling pillows, vaginal moisturizer, and sleep support supplements.
- Health Savings Accounts are a great way to provide a tax-advantaged approach to covering the cost of HRT medications, nutritionist visits, and appointments with menopause trained gynecologists.
- Mental health support is for all stages of life, but particularly important during menopause. Menopause is on the list of mental health support provided and Mona feels more comfortable seeking care because the stigma has been removed around menopause in the workplace.
- The hormonal fluctuations women experience in menopause can impact their vision. Mona makes sure to get her annual eye exam because her vision is blurred.
- The Calm app offered allows Mona to practice mindfulness and stay in the moment to stave off a hot flash or irritability.
- She is entitled to sick days under the company policy and applicable laws, and can use them for menopause symptoms or doctor’s visits.
And while menopause is often framed around cisgender women, it’s important to note that transgender women can experience symptoms too. To assist in their medical transition, trans women are typically prescribed estrogen and sometimes progesterone, and can take hormone replacement therapy as well. If these therapies are reduced or interrupted, the ensuing hormonal fluctuations can lead to menopausal symptoms like hot flashes. (Just as trans women taking hormones can experience PMS-like symptoms in their younger years.)
Step two: Think about whether some policies or benefits should be augmented, or new ones created
As you go through Mona’s journey, we may also come upon areas where we aren’t supporting her as much as we could. In some companies, we may have the ability to add new policies. Of course, these aren’t one-size-fits-all, but rather thought starters for companies seeking to augment their current benefits. These could include:
- “Dedicated leave: Some companies in the UK are doing this. Companies in the US can consider adding this to their current sick leave policy, or adding dedicated days off. How amazing for Mona to know that her company sees her, and has offered her the option of taking a few days off to recoup much needed sleep.
- “Flexibility: A flexible work schedule, when possible, or arrangements that include work from home may benefit Mona during this time. Consider recommending in the handbook that women experiencing menopause connect with their HR partners, who can help them navigate solutions that may include job-sharing, temporary part-time options, etc.
- “Specialized healthcare benefits: More employers are offering specialized telehealth services, and menopause doesn’t need to be an exception. Gennev works with insurance companies to provide in-network benefits, which are often paid for by a combination of the employer and insurance.
Step three: Train staff
Once you have identified existing benefits and policies, or created new ones, it’s important to train HR business partners, or key HR contacts, in menopause support. Ensure they understand what is in the benefits package and company policies. Gennev offers webinars that can educate HR teams on menopause symptoms, how to respond sensitively to requests and how certain accommodations can help.
Step four: Communicate widely to your employees
If Mona doesn’t know what tools are available to support her, she can’t take advantage of them. Consider adding to your benefits documents or company policies a section specific to menopause, entailing how Mona can take advantage of existing benefits and policies, and including any new ones.
When you present the benefits package to the company, call this out specifically. Consider a slide detailing the benefits and policies that apply to her.
Physical improvements and accommodations
It’s not always possible to improve physical space, but even small changes can be a big help for women in menopause. Some potential steps to take:
- Review temperature control in your workspace, and as possible, allow employees to make changes, or to work with HR to make changes, in their work area.
- Consider creating a “cooling room,” where anyone experiencing hot flashes from menopause or other causes can recover privately, or with others experiencing the same symptoms. This room can be kept cooler than the rest of the office. Consider making a mini-fridge with ice packs available. HR can grant access to that room.
- Provide employees with fans and cooling pillows upon request.
Education and company-wide conversations
Discussing menopause carries a great stigma. Women themselves are not always educated on what’s happening. It’s also important that people managers are prepared to support employees “ not just the HR department.
Consider the following resources for women in menopause:
- Start an employee resource group (depending on the size of your company). This should be employee-led, but there are models for this at many companies.
- Provide webinars and other educational opportunities for women in menopause. These can be through a dedicated menopause clinic, like Gennev, or through other sources.
For the company as a whole, some potential actions are:
- Include a section for existing leadership, or in sensitivity training, on menopause, its symptoms and how to support fellow employees experiencing it.
- Provide webinars or other training for people managers, like those offered by Gennev, that discuss how to best support Mona.
Make a Difference
Companies today are embracing inclusivity, which comes in many forms “ and ages. The most happy and high-performing workplaces proactively support their employees’ well-being, and are generously understanding. Providing support services for women experiencing menopause is not just kind, it’s smart business. Addressing menopause will increase employee collegiality, productivity and retention, and help all employees to maintain the full potential that they strive to achieve.
“
Menopause is the permanent cessation of menstruation and a natural part of a woman’s life. However, for some women, menopause doesn’t happen naturally. Surgical menopause is the removal of a woman’s ovaries, which results in immediate menopause. Though symptoms of menopause are similar whether it occurs naturally or surgically, the experience is often more difficult following surgical menopause”but there are ways to make it more manageable.
Menopause typically happens gradually, with hormones fluctuating and symptoms waxing and waning. It’s a transition that can take anywhere from about four to ten years and begins with perimenopause. During this time, estrogen and progesterone, the primary reproductive hormones, are declining, which causes irregular periods, one of the first signs of perimenopause. Other common symptoms include hot flashes, trouble sleeping, mood swings, and brain fog.
What is surgical menopause?
Surgical menopause occurs when both of a woman’s ovaries are removed, a procedure known as an oophorectomy. “There are some very good reasons to remove both ovaries,” says Dr. Lisa Savage, board-certified OB/GYN, and Gennev clinician. The most common are a cancer diagnosis, a high risk for cancer, and endometriosis. Removing both ovaries is a bilateral oophorectomy and can be lifesaving for some women with cancer or a high risk of developing it, or in the case of endometriosis, it could significantly improve a woman’s quality of life. (The removal of only one ovary is a unilateral oophorectomy.)
The ovaries produce estrogen and progesterone, so when they are removed, these hormones are gone, too. “Surgical menopause is this abrupt cessation of those ovarian hormones, whereas naturally-occurring menopause is more of a transition,” says Dr. Savage. “The transition may not be a picnic, but an abrupt cessation can be more intense, especially in younger women.”
Risks of surgical menopause
After the removal of your ovaries, you may experience more symptoms that appear immediately following surgery and are more severe, compared to perimenopause, where symptoms ebb and flow over a longer time period. So instead of your body being gradually weaned off of estrogen and progesterone, it’s like going cold turkey. The withdrawal can be tough. Suddenly, you could be hit with hot flashes, sleeplessness nights, mood swings, and low libido all at once or some combination on top of recovering from your surgery. And the intensity of these symptoms may be higher than if you gradually entered menopause. Like natural menopause, though, the types of symptoms and their severity vary from woman to woman.
Surgical menopause also has long-term effects that differ from natural menopause. When you go through menopause, you lose the protective effects of estrogen that particularly benefit your heart, bones, and brain. Heart disease risk increases. Bone loss may be accelerated. Cognitive function can be affected, and your risk of dementia and Alzheimer’s may rise. The average age of natural menopause is 51, and it’s after menopause that these problems tend to arise. If you have surgical menopause at an earlier age, things happen sooner.
“It’s double jeopardy if you lose your ovaries at a young age,” says Dr. Savage. “You have more years to live without estrogen and more time to develop those problems. More time of estrogen deficiency is worse than less time of estrogen deficiency.”
But there are ways to minimize the effects if it’s necessary to remove both ovaries. Sometimes you can have only one ovary removed (unilateral oophorectomy) or keep them both, based on your personal situation. That’s why it’s essential to talk to all of your doctors about your options and consider getting a second opinion whenever you’re having surgery.
What happens after a hysterectomy?
“A hysterectomy does not directly induce menopause,” says Dr. Savage. A hysterectomy is the removal of the uterus. Just because you had a hysterectomy doesn’t mean your ovaries were removed.
In the past, a hysterectomy often included an oophorectomy for women nearing menopause, partly to prevent ovarian cancer. The latest research, however, shows that ovarian cancer more likely originates in the fallopian tubes, and there are benefits to keeping the ovaries. “Now, we may routinely remove the fallopian tubes at the time of a hysterectomy for benign indications but leave the ovaries because they may not be the primary source of “ovarian’ cancer,” says Dr. Savage.
If your uterus is removed, but you still have your ovaries, you’ll stop menstruating, but your ovaries will continue to produce hormones. That means you won’t experience perimenopause until ovarian function declines. For some women, who’ve had a hysterectomy, the decline will follow a similar timeline as women who still have their uterus. However, sometimes it occurs sooner.
“The blood supply to the ovaries can be compromised during a hysterectomy because some of the blood supply is common to the area,” says Dr. Savage. “That doesn’t mean anything was done wrong. It can be a natural consequence of a hysterectomy that ovaries cease functioning earlier than they might have otherwise.”
Communication with your physician is key
No matter what type of surgery you’re having, you should understand the procedure, your options, possible side effects, and the recovery process. It is even more critical if your doctor recommends removing your ovaries. “It’s very important that women talk to their surgeons in detail as to exactly why they want to remove the ovaries,” says Dr. Savage. “Make sure there’s a good indication for removing them, and there may be. If not, advocate to keep your ovaries.” You might even want to get a second opinion. “I tell patients if they need a hysterectomy for a benign condition go to the mat to keep their ovaries,” Dr. Savage says. One ovary is usually sufficient to produce enough hormones to prevent you from going into menopause early.
If your ovaries have to go, the conversation with your doctor should shift to managing the impending menopause. “Have a plan in place preoperatively,” says Dr. Savage. “Don’t wait and be reactive. Knowing what to expect ahead of time is so empowering.”
How to manage surgical menopause
Just like natural menopause, some women who have surgical menopause have an easier time than others. Even if your symptoms are mild, surgical menopause requires management, especially the younger you are. “It’s not just about hot flashes,” says Dr. Savage.
Estrogen plays a role in nearly all your body systems, including your skin, hair, and vaginal tissue. More important is its effect on your heart, brain, and bones. Estrogen protects the heart, fuels brain activity, and strengthens bones.
When you no longer have estrogen, your risk of heart disease increases, cognition may decline, mental health issues like depression and anxiety are more common, and bone loss increases. It can also have a significant impact on your sex life. Vaginal dryness and a loss of libido can be more pronounced following surgical menopause. And the longer you are estrogen deficient, the more problems you can have. “With life expectancy into your 80s, you must take care of those body systems to carry you through,” says Dr. Savage. “You want them working well for the rest of your life.”
Here’s how to manage surgical menopause and stay healthy as you age.
Ask about hormone replacement therapy (HRT). Talk to your doctors to find out if you’re a candidate. The answer will depend upon your individual situation, including the reason for having your ovaries removed. There are some contraindications, for example, if you have estrogen-dependent breast cancer. Discuss your options with all of your doctors. “Any replacement that you take up to the age of 51 is just replacing what you should have had anyway,” says Dr. Savage.
Start HRT quickly. If you are a candidate for hormone therapy, you want to start as soon as is safe following your surgery. “You shouldn’t have to wait to feel terrible to be put on replacement therapy,” says Dr. Savage. “It’s like having your thyroid out and getting replaced quickly.” Dosages might need to be higher in younger patients to achieve physiologic levels of premenopausal estrogen. If you still have your uterus, you’ll also need progesterone to prevent an overgrow of the uterine lining which could become cancerous.
Explore other medications. If you’re not a candidate for hormone therapy, there are other options. Some SSRI (selective serotonin reuptake inhibitors) anti-depressants like Effexor and gabapentin, an anti-epileptic medication, have been shown to help with menopause symptoms, especially hot flashes and night sweats. A new, nonhormonal drug Veozah was recently approved to treat these symptoms. Other medications can reduce your disease risk.
Monitor risk factors. You’ll want to be proactive about disease prevention, so talk to your doctor about prevention strategies and screening tests. You may need cardiac evaluations or bone density tests at an earlier age. If your risk increases, for example, your cholesterol or blood pressure levels rise, or your bone density decreases, quickly addressing those issues will be critical.
Make lifestyle changes. All of the advice that can help with natural menopause, such as exercising, staying hydrated, eating more fiber, taking supplements, and reducing stress also apply to surgical menopause.
Take care of your mental health. Sudden menopause can be more intense psychologically, so seeking helpis essential. Mood swings, anger, and anxiety are common with any type of menopause. With surgical menopause, these symptoms can be more severe, and you may be dealing with other issues like a possible a cancer diagnosis that can add more stress.
Surgical menopause requires management by a trained menopause specialist. Speak with one of Gennev’s board-certified OB/GYNs to learn more about managing symptoms, and stay healthy as you age.
“
You are not going crazy! You may feel as if you’re going crazy at times”or most of the time”but you’re not. Whether you’re experiencing more angry outbursts, down-in-the-dump moods, frazzled thinking, or more severe distress, know that it is not just in your head.
“Many women are shocked by the mood swings, anger, and anxiety that can start in the perimenopause,” says gynecologist Rebecca Dunsmoor-Su, M.D., chief medical officer at Gennev.
Instead of simply ignoring a quirky habit that your partner has, like you used to do, you now blow. And then, after a heated argument about something that, in the grand scheme of life, isn’t important, you feel guilty and wonder what’s wrong with you. Or maybe the nervousness you used to have about public speaking now becomes a full-blown panic attack. “It is due to the way the brain responds to the hormone swings that happen naturally during this time, but that does not make you simply hormonal,” says Dr. Dunsmoor-Su. “The symptoms can be even worse if you are someone who has these at baseline.”
Mental health issues are real and common in perimenopause and menopause, but there’s help. You’re not alone. And, you don’t have to suffer through it alone.
In general, women experience mental health problems at a higher rate than men”1 in 5 women compared to 1 in 8 men. The incidence increases during the menopausal years. One in three women, ages 50 to 64, reported needing mental health care in the past two years, according to the 2022 Kaiser Family Foundation Women’s Health Survey.
How does menopause affect mental health?
It’s completely normal to feel more emotional or have a harder time controlling your emotions during this stage of life. Along with the usual life stresses, women’s relationships are often shifting at this time. Their kids are leaving home. Parents may require more care. “All those things are going to impact a woman’s mental health,” says Dr. Dunsmoor-Su.
And then add in a rollercoaster of hormones. “The brain is exquisitely sensitive to estrogen and progesterone,” says Dr. Dunsmoor-Su. “It’s had these hormones in a particular pattern its whole life, and now that pattern is broken. The brain is behaving differently because the pattern is different.” And the pattern keeps changing, resulting in different symptoms as you progress from perimenopause to menopause.
Mental health in perimenopause
Perimenopause is the two- to 10-year transitional period to menopause when a woman stops menstruating. During perimenopause, though, a woman is still getting her periods, but they may be more erratic. Every month, there is a surge of estrogen in the first half of the cycle and a surge of progesterone in the second half. The ovaries are still producing eggs, but more estrogen is needed to stimulate them. Through the cycle, estrogen levels get higher, progesterone levels increase to match the high estrogen, and then all of the hormones drop. “You get really big spikes of hormones,” says Dr. Dunsmoor-Su. “You get really big troughs of hormones. It’s a roller coaster of hormones, and the brain doesn’t like roller coasters. The brain likes nice, sedate walks on a path.”
These drastic fluctuations often predispose women to anxiety, anger, and mood swings. Some women also experience depression or worsening of their symptoms if they already had depression before perimenopause. Those symptoms may also be worse for women who’ve previously experienced premenstrual syndrome (PMS) or its more severe counterpart, premenstrual dysphoric disorder (PMDD). The good news is that these mental health issues tend to be temporary symptoms associated with perimenopause. As your hormone levels decline and fewer fluctuations occur, mood swings and anxiety often lessen. However, depression can be more common after menopause.
Postmenopausal mental health
Menopause is achieved once you’ve gone 12 months without a period. “In post-menopause, there is very low estrogen and basically no progesterone,” says Dr. Dunsmoor-Su. The decline in hormones tends to level out mood swings, ease anxiety, and tame anger, but can be associated with an increase in depression. In addition to the effect of hormones on your mood, other frequent postmenopausal issues such as hot flashes, poor sleep, body changes, and stress can all contribute to depression. Studies associate increased hot flashes with increased depression. Symptoms are often worse for women who’ve had depression at other times in their lives. And 15 to 20 percent of women may be diagnosed with new-onset depression in midlife.
Unlike anxiety and mood swings, which tend to resolve once you’re postmenopausal, depression may stick around. “If you’re someone who has had depression your whole life, you may get a temporary exacerbation through the menopausal transition, and then it might get somewhat better,” says Dr. Dunsmoor-Su. “These things wax and wane.”
Despite these general patterns in mental health symptoms during midlife, the experience can differ from one woman to the next. “It’s a fluid time,” says Dr. Dunsmoor-Su. “Every woman’s journey is different. They’re going to go through the same hormonal changes, but the way their brain behaves is very different because of the different patterns of estrogen and progesterone receptors in the brain.” And because women’s menopause experiences vary, treatments can vary, too.
When to get help for your mental health
Immediately! As women, we tend to take care of everyone else first and often put our needs aside. But this strategy isn’t helpful for anyone over time. Think of it this way, what would be the most effective way of saving your loved ones if you were all in a leaky life raft? You’d wear yourself out and wouldn’t save anyone if you’re madly bailing the water. But if you take the time to patch the leak, you’ll save everyone without sacrificing yourself.
“Menopause is already a stressful time on the body, says Dr. Dunsmoor-Su. “It impacts your long-term health, sense of well-being, cardiovascular health, and longevity. It’s important to care for yourself because this is the beginning of the rest of your life. You’ve got a solid 30 to 40 more years to live, and you want to do it in the healthiest way possible. If you don’t address your sources of stress, mental health being one of them, it can be harder to live a healthy life.”
Now isn’t the time to try to push through it or let the stigma of mental health issues prevent you from seeking help. If you notice that any of these mental, psychological, or emotional issues are impacting your quality of life, you should talk to your doctor or healthcare provider. Common signs that it’s time to take care of your mental health may include feeling less able to manage day-to-day, negative changes in relationships, problems at work, a lack of desire to participate in activities that you used to enjoy, or others noticing a difference in you.
If any of these apply to you, talk to your primary care doctor, gynecologist, or menopause doctor. Let them know that you’ve noticed these changes in your mental health and want to know what resources are available. You can also ask for a referral to a mental health professional.
Sometimes mental health issues can be severe and require immediate attention. According to a European epidemiological study across the reproductive life cycle of women, suicidal ideation increases during the menopause transition. The study showed a 7-fold increase in suicidal ideation in perimenopause versus other women. If you are experiencing any thoughts about hurting yourself or others, seek help right away.
Treatments for mental health problems in menopause
As menopausal mental health problems differ from one woman to another, so do treatments. The course of action often depends on the severity of symptoms and can range from lifestyle interventions or therapy to hormone therapy or medications.
Sometimes treating physical symptoms like hot flashes or sleep problems can improve your mental health without additional treatments. But if you need something more, there are lots of options.
During perimenopause, low-dose birth control pills may be enough to quell mild to moderate anxiety, depression, and mood swings. “There is some good data that in perimenopause hormone therapy is as effective as SSRIs (the most common antidepressants such as Prozac) for managing depressive and anxiety symptoms,” says Dr. Dunsmoor-Su. For postmenopausal women, a combination of estrogen and antidepressants works better than either alone, according to research.
Therapy is another option that may complement other treatments or work on its own. “Having behavioral techniques that you can use when you’re feeling very stressed or anxious can be really helpful during this time,” says Dr. Dunsmoor-Su.
“We have to look at each patient as an individual,” she says. “One patient may need mental health care. One patient may need hormones, and one patient may need both. It’s about taking a holistic look at the patient and her symptoms and figuring out how we can help.”
You deserve the best care for your physical and mental health in menopause. Together with LifeStance Health, one of the nation’s largest providers of virtual and in-person outpatient mental healthcare, Gennev offers access to menopause-trained OB/GYNs, psychiatrists, psychologists, licensed therapists, and dietitians who provide guidance, prescription support, and lifestyle therapies for your mind and body through this important stage of life.
“Learn more about how Gennev patients receive integrated care that addresses both the physical and mental health symptoms associated with menopause.
“
If your concerns feel too heavy to handle, there is no shame in seeking professional help: Call, text, or chat 988 to reach the National Suicide Prevention Lifeline, and you will be connected to trained counselors that are part of the existing Lifeline network. You can also dial 800-273-8255 or chat via the web at 988lifeline.org/chat/.
“
The information on the Gennev site is never meant to replace the care of a qualified medical professional. Hormonal shifts throughout menopause can prompt a lot of changes in your body, and simply assuming something is “just menopause” can leave you vulnerable to other possible causes. Always consult with your physician or schedule an appointment with one of Gennev’s telemedicine doctors before beginning any new treatment or therapy.
“
This twist on traditional hummus is sure to please. The edamame packs a huge plant based protein punch. And added bonus – soybeans (edamame) contain isoflavones, a type of phytoestrogen that may reduce the frequency of hot flashes in some women. It’s full of fiber and healthy fat (from the olive oil and tahini), making this a high-satiety snack. We love to pair it with some raw cut veggies or whole grain pita triangles.
Edamame Hummus Recipe
Serves 8 (¼ cup servings)
Adapted from Cookie and Kate food blog
Ingredients:
- â cup tahini
- â cup lemon juice (about 2 to 3 lemons)
- 3 tablespoons extra-virgin olive oil, plus more for garnish
- 1 medium clove garlic, roughly chopped
- ½ teaspoon fine-grain sea salt
- ½ cup lightly packed fresh cilantro leaves, plus more for garnish
- 1 ½ cups shelled edamame (10 ounces), defrosted if frozen
- 2 to 4 tablespoons water, as necessary
- Sesame seeds for garnish (optional)
Instructions:
- Place all ingredients in a food processor and process until smooth. Adjust water as needed until you reach the desired consistency.
- Garnish with sesame seeds or edamame.
- Serve with cut veggies, crackers or pita.
“
Looking for more healthy recipes, or guidance on how to incorporate healthy recipes like this and others into your diet on a regular basis? Consider working with our integrated care team of physicians and Registered Dietitians who are experts in supporting women in menopause. They will create a personalized plan to optimize your nutrition and other lifestyle factors, plus provide you one-on-one support to create healthy habits for the long-term.
The fresh start that each new year brings also offers a chance to renew your commitments to the business of your health. While you are setting your health-first intentions for the upcoming year, this handy “Health Checkup Checklist” may help you focus on the preventive care and screenings that can give you the edge when it comes to your health.
The changes in your body in the years surrounding menopause may cause you to experience not only new symptoms associated with hormone fluctuations, they may also increase your risk for health conditions such as heart disease, diabetes, cancer, and osteoporosis. With regular screenings you will be well-informed of your risk factors, and be poised to implement prescribed preventive or defensive measures.
Getting your appointments on the calendar is half the battle. But many providers have made that easier than ever with online appointment scheduling. So, no excuses! As the saying goes, “an ounce of prevention is worth a pound of cure”.
Make these a must-do every year!
Your Annual Wellness Visits as At the top of your list of important appointments this year will be with your primary care physician (PCP) and your gynecologist for your wellness check-ups. This is where, together with your provider, you will review your current health and risk factors, and determine your personal disease prevention plan.
With your PCP, you can expect to have a blood pressure check and bloodwork, plus advice on vaccinations not only for flu and virus, but also tetanus booster or shingles vaccine. Your PCP can also help you check the boxes on referrals for many of the screenings that you are due (or overdue) for.
Your annual gynecological appointment may include a pelvic exam, cervical cancer screening, and a breast exam. And while some PCPs are willing to perform breast and pelvic exams and do Paps, the focus and expertise of a gynecologist is of benefit and added value when it comes to receiving the most comprehensive women’s healthcare.
Dental Care as Seeing your dentist twice a year for routine cleaning appointment and screening for teeth and gum disease doesn’t just care for your teeth, it also protects your health. Inflammation in your mouth can allow bacteria to enter the bloodstream causing inflammation elsewhere in the body. This is why gum disease is linked to many chronic conditions including heart disease, diabetes, respiratory illness, osteoporosis and rheumatoid arthritis.
Eye Checkup as Depending upon your individual health history, a routine eye exam is recommended every one to two years. An optometrist or ophthalmologist will check for signs of eye disease including glaucoma, cataracts, and age-related macular degeneration.
Skin Cancer Screening as Individuals with average risk will want to plan for a yearly visit with the dermatologist for a skin cancer screening and examination of any moles, spots or lesions. If you have a family history of skin cancer or have other underlying risk factors, your doctor may recommend more frequent visits.
Start these screenings at age 45 (if not before)
Menopause Check-up (Gennev refers to this as the M-check) – Starting at the age of 45, women’s post reproductive health care begins with a menopause check-up. A board-certified OB/GYN who specializes in menopause will answer the health pains of menopause, determine what state of menopause you currently are in, and may help assess the risks for chronic issues that may arise as your estrogen declines. The incidence of rising cholesterol, depression, sexual dissatisfaction, fluctuating blood sugar levels and more are common after menopause, and it’s best to address these changes before they become health concerns. If you haven’t had your M-check, start by taking the assessment. Then, speak with a doctor and feel better starting now.
Mammogram as The American Cancer Society suggests that women with no prior history, or family history of breast cancer get mammograms each year beginning at age 45, and continue with screenings as long as a woman is in good health and is expected to live 10 more years or longer.
Colonoscopy as Due to the increase in colorectal cancer in younger individuals, The American Cancer Society now recommends that screenings for individuals with average risk begin at age 45. Colonoscopies can detect disease, and may help prevent cancer as precancerous polyps can be removed during the procedure.
Bone Density as Osteoporosis often begins to develop in women a year or two before menopause. For this reason, working with your physician on when a DEXA scan may be right for you is important. The current national recommendation for individuals with average risk is to do a DEXA scan at 65. But for menopausal women with a fragility fracture or strong family history, earlier screening may be recommended.
Put your best foot forward with healthy lifestyle changes
With your health and well-being being top of mind, there’s no better time to recommit to the daily habits that support your body and mind during menopause and beyond.
- “Feed your body right – Menopause brings with it many bodily changes, but a well-balanced diet and nutrition can help support you on your journey. Learn more with Nutrition Recommendations for the Menopause Transition.
- “Re-examine your alcohol intake as When you reduce or remove alcohol from your diet, the health benefits quickly add up. Find out ways to help curb your urge for cocktails.
- “If you smoke, STOP! as Cigarettes can amplify what is already bad about menopause. Check out these tips for how to quit for good.
- “Sleep better as A good night’s sleep has restorative powers. Read more with a Woman’s Guide to a Good Night’s Sleep.
- “Move every day as Daily exercise can help reduce the risk of diabetes and heart disease and slow bone loss after menopause. And walking is one of the easiest steps you can take to keep moving! Learn more about the Benefits of Walking.
Whether you’re in perimenopause or post-menopause, lifestyle behavior change is a must for managing weight, hot flashes, anxiety, sleep, fatigue and joint pain. Gennev’s menopause specialists work with women of varying levels of discipline, so don’t overthink it, just start by doing something. Put your health first this year, and book an appointment.
The information on the Gennev site is never meant to replace the care of a qualified medical professional. Hormonal shifts throughout menopause can prompt a lot of changes in your body, and simply assuming something is “just menopause” can leave you vulnerable to other possible causes. Always consult with your physician or schedule an appointment with one of Gennev’s telemedicine doctors before beginning any new treatment or therapy.
Perhaps you’ve heard of Shakshuka? Maybe you have seen it on a menu or picked up the frozen version at Trader Joe’s. This flavorful, healthy recipe is easy to make, and is a favorite of ours here at Gennev. We’ve even had Gennev Registered Dietitian, Monika Jacobson guide us through making shakshuka from our own kitchens via a virtual zoom cooking class. We all loved it and now many of us make this dish on repeat!
Shakshuka is a traditional dish from Northern Africa or the Middle East, made by poaching eggs in a flavorful tomato stew full of spices. It is loaded with vegetarian protein (eggs and cheese), anti-inflammatory spices, vegetables (microgreens, tomatoes, onions) and healthy fat (avocado, olive oil).
Shakshuka beautifully aligns with the nutrition concepts our Registered Dietitian Nutritionists teach, as it fits within a Mediterranean-style diet. It’s typical to enjoy shakshuka as a breakfast meal, but it can also be a lovely holiday brunch food or an easy weeknight dinner any time of year.
This ethnic comfort food offers delectable flavor, superb nutrition and is easy to make! Give it a try this month or save it as a healthy meal for another time.
Shakshuka Recipe
Adapted from Love and Lemons
Ingredients
- 2 tablespoons extra-virgin olive oil
- 1 cup chopped yellow onion
- 1 red bell pepper, seeded and diced
- ¼ teaspoon sea salt, more to taste
- Freshly ground black pepper
- 3 medium garlic cloves, minced
- ½ teaspoon smoked paprika
- ½ teaspoon ground cumin
- Pinch of cayenne pepper, optional
- 1 28-ounce can crushed tomatoes
- 2 tablespoons harissa paste
- 1 cup fresh spinach, chopped
- 3 to 5 eggs
- â cup crumbled feta cheese
- ¼ cup fresh parsley leaves
- 1 avocado, diced
- Microgreens for garnish, optional
- Toasted bread, for serving
Instructions
- Heat the oil over medium heat in a 12-inch lidded stainless steel or enamel-coated cast-iron skillet. Add the onion, red pepper, salt, and several grinds of fresh pepper and cook until the onion is soft and translucent, 6 to 8 minutes.
- Reduce the heat to medium-low and add the garlic, paprika, cumin, and cayenne, if using. Stir and let cook for about 30 seconds, then add the tomatoes and harissa paste. Simmer for 15 minutes until the sauce is thickened.
- Add the spinach and stir until wilted. Make 3 to 5 wells in the sauce and crack in the eggs. Cover and cook until the eggs are set, 5 to 8 minutes. The timing will depend on how runny you like your egg yolks.
- Season with salt and pepper to taste and sprinkle with the feta, parsley, avocado, and microgreens, if using. Serve with toasted bread for scooping.
Proper nutrition is key to warding off disease as we age. If you need guidance on how to incorporate healthy recipes like Shakshuka and others into your diet on a regular basis, consider working with our integrated care team who are experts in supporting women in menopause. They can create a personalized plan that will optimize your nutrition and other lifestyle factors, plus provide the support to create healthy habits for the long-term.
“
While menopause is a normal and natural part of aging for women, many of us have no idea what to expect as we approach our post-reproductive years. And many symptoms that can accompany menopause, along with their impact on our bodies, minds and emotions, can leave even the strongest woman feeling alone. Because the topic of menopause was, and is, still widely considered “taboo” or “off limits” for our mothers, and our mother’s mother (and so on), many of us find ourselves part of a tribe of women lacking the passed-down knowledge that could make all the difference for how we approach this inevitable time of our lives.
One of the most powerful aspects of the Gennev brand is the community of women who gather with us, finding common ground with other women through shared experiences, offering advice and gaining support from someone who “gets it”. We have made it our mission to educate women about menopause. Our wish is that women will be part of the change, and help us pass on menopause knowledge to future generations.
We asked the Gennev community what advice they would share with younger women about what to expect in menopause. Below are their responses.
It’s so much more than hot flashes
“First of all, it is important to talk about strange symptoms you are experiencing. Ask questions, do not be ashamed and see a trusted GP that will help you through it. Be brave and know that you are not alone”¦” Mauricia B, 48 Perimenopause
“Menopause is NOT just about hot flashes. There are a lot of symptoms to consider that can impact your long-term health during perimenopause and menopause. I started experiencing perimenopause at age 43 and left it to fester until it was unbearable at age 49. I wish I had taken it seriously while I was knee-deep in perimenopause.” Valerie W, 58, Postmenopause
“Menopause is so much more than just not having a period. It involves the mind and the body and the changes are different for everybody. It’s important to take very good care of oneself, eat properly, continue to move and exercise and to keep the brain active. I would recommend trying the least invasive things first to relieve uncomfortable menopausal symptoms. If that doesn’t work then try hormone replacement therapy and keep checking in with yourself. It helps to discuss menopause with other women that are going through or who have been through similar circumstances.” Terry C, 56, Postmenopause
“It’s a natural progression in the life of a woman. Learn as much as you can in your thirties so that you’re prepared and aren’t overwhelmed by the changes that will take place physically, mentally, and emotionally. Talk to other women about their experiences if they’re open to it.” Anonymous, 63, Postmenopause
“It creeps in on you and starts earlier than you might expect”¦!” Anonymous, 49, Perimenopause
Don’t suffer through symptoms, and seek menopause care
“If you have an OBGYN, expect to explore a gynecologist with specialty in menopause. Doctors are never taught menopause. And they themselves don’t know very much about it for themselves. Don’t expect the doctors to have the answers. They don’t. Mine told me I was crazy – what I’m experiencing is due to stress, travel, work, etc. Not perimenopause even though I knew in my gut that this wasn’t just life circumstances and choices. It was a shift in my body make up. Trust your intuition.” Anonymous, 46, Perimenopause
“Hormones havoc the lives of women to such an extent that we find no road, but stay calm, till the symptoms subside on their own – it might take years of our life, nothing is in our hands except the lifestyle changes and positive approach towards the transformation we have.” Anonymous, 50, Postmenopause
“Don’t suffer with symptoms; blood tests do not give the full picture; arm yourself with information.” Anonymous, 45, Perimenopause
“It has helped me to just dive into learning about it. I’m also reminded of the quote that goes something like “the only thing certain in life is change”. I’m working on embracing and finding the positives in the changes. For me, getting to this stage of life means I have a lot more freedom and options of how I spend my work time and free time. That’s definitely a positive aspect of all of this!” Anonymous, 42, Perimenopause
“Expect that you will probably be in perimenopause long before you think you are, and that even if you have a female doctor, they might not be able to give you the correct or all the information you need. They may not know any better of what is happening to you. So, READ whatever you can about perimenopause, menopause, etc. Don’t be afraid to talk with your friends. I’ve found that when I bring up what I’m going through, so many of them are willing to open up and seem almost relieved to have someone else to talk to. You’re not alone!” Lisa H, 50, Postmenopause
“Expect! I’d tell all start now! Ask your mother and also if you have a grandmother, your aunts. Plain as can be I say look for reputable menopause research.” Ginny K, 63, Postmenopause
“Totally natural process but there are so many different ways each woman goes through it. For me having a close friend also going through it helps. We talk to each other about it also.” Annalise S, 46, Perimenopause
“Expect your body’s “normal” patterns to change – some changes will be annoying and frustrating and some will be a relief. Don’t freak out but do check in with your doctor because there might be something else exacerbating your symptoms. Embrace the transition from being the fresh-faced newbie into being the mentor who can give wise guidance. You have a lot to offer the world even if no one else is validating that right now. Your creative energy may shift in a new direction and that is okay. It’s okay to stop chasing youth and embrace your scars, and grey hair, and laugh lines – let your character show.” Angela S, 47, Perimenopause
“Everyone’s body is different and will experience different symptoms. When you feel like you’re at your ropes-end, press forward with all you got.” Anonymous, 43, Perimenopause
“Read, learn, discuss with those who you know who have experienced it because it WILL happen to you.” Jennifer F, 53, Perimenopause
“It is different for everyone. You are unique and need to know yourself and your body. Reach out for help. Hormones are real. They do run our lives ….. :-)” Lisa J.B., 53, Perimenopause
“Hot flashes are no joke, so dress in layers. And, don’t be ashamed or afraid to talk about it. Menopause was always something I thought of happening when I’m “old” but at 52 I’m not old at all. I’m healthy, vibrant, fun & fun-loving. I’m strong and sexy and smart. It can certainly be a bit of a roller coaster, but talking about it, sharing your experience and finding some humor in it can all be healthy and therapeutic in managing it. And the more we, as women, talk about it the more it’ll become “normal” vs taboo or something that signals “old age”. It’s just a stage that we all go through. And the best part? Never having to worry about your period again. You can wear whatever you want, white pants and all, whenever you want! Not gonna lie though, I’ll be glad when the hot flashes are over…” Erin E, 52, Postmenopause
“Expect your journey to be your own. Expect to get help so demand it. Expect to be amazed and empowered by the women you’re in it with!” Jenn K, 50, Perimenopause
“I would advise to expect a period like your teenage years with a lot of hormones imbalance so I would advise them to get ready early as possible with lots of information to be able to prepare your body and your mind, and don’t think of menopause as a taboo because it doesn’t represent the end of our life or something to be ashamed of. And I really hope that soon GPs could be more knowledgeable about it and be more supportive because we really need it.” Orietta F, 52
“Read all you can about it. It’s been really rough for me, but knowledge has helped me know how to help myself.” Paula C, 50, Perimenopause
“Be aware that any physiological and/or psychological changes from your mid 30s could be hormone-related. The symptoms of perimenopause are so wide-ranging and vary from woman to woman but, certainly, if you were previously a happy, optimistic person and suddenly realize you are feeling low and/or anxious for no particular reason, this could be a sign that things are starting to change.” Louise S, 44, Perimenopause
“Take extra good care of all parts of yourself. Emotionally, physically and spiritually. Address underlying issues, don’t let things be swept under the rug.” Tanya C, 53, Perimenopause
“Don’t dread it, but instead inform and arm yourself with information and stories from other women. Women don’t need to suffer; there are so many ways to feel really amazing in your body. This time of life is too precious not to live to your fullest.” Jill A, 47, Perimenopause
“I was afraid to talk about it. My kids were in their late teens and early twenties, every time the “M” word came up they would tease and joke about it excessively. I would not talk about it, but I finally got fed up and told them it was hurtful and isolating. That changed the entire concept of menopause for all of us. I did not want to be “old” enough to be perimenopausal! Acceptance made the process so much easier.” Dana H, 52, Postmenopause
“Find someone supportive to talk/cry/laugh with. My sister and I lean on each other.” Lisa C, 57, Postmenopause
“Be good to yourself, even though it’s hard, embrace the changes in your body and try to deal with relations issues as best you can before you are officially in menopause. I found the things I didn’t deal with before in my life came at me bigger and worse than ever. Really had to cut some ties this year, grieve a lot and make time for myself to stay as calm as possible.” Laurie C, 59, Postmenopause
“It can start as early as your 30’s. Talk with your mother/aunt/grandmother about the issues they experienced. Educate yourself and empower every young woman to do the same.” Deborah B, 57, Postmenopause
“When you start to experience symptoms that aren’t “you” – brain fog, irritability, low energy, mild depression, increased anxiety, wonky periods – don’t let your provider tell you: “You’re too young to be experiencing perimenopause.” Go online and search for a provider that specializes in menopause symptoms and treatment, because you’re going to need her expertise for the next decade or more. Starting early will mean you’re not caught unaware and alone in the journey every woman takes. You will have education and support.” Dessie, 51 Perimenopause
Be part of the change in educating women about menopause
Join us in being part of the change! Share these 28 responses along with your own menopause experiences with the younger women in your personal community. We all menopause better together!
There are over 34 symptoms that women experience throughout menopause. From hot flashes, weight changes and sleep disturbances, to vaginal dryness, mood swings and fatigue, hormonal shifts are something you can expect in menopause! There’s no need to grin and bear the symptoms of menopause. Gennev’s board-certified OB/GYNs specialize in menopause and will help you understand your symptoms and find relief with prescription or natural therapies that are right for you.
“
The information on the Gennev site is never meant to replace the care of a qualified medical professional. Hormonal shifts throughout menopause can prompt a lot of changes in your body, and simply assuming something is “just menopause” can leave you vulnerable to other possible causes. Always consult with your physician or schedule an appointment with one of Gennev’s telemedicine doctors before beginning any new treatment or therapy.
“
When we asked women this past year what they knew about menopause before starting their own journey, their answers were overwhelmingly, “not much”. Beyond hot flashes and night sweats as well as no more periods, many women were unaware of what to expect, and were caught by surprise by the widespread impact on their bodies and emotions. One woman commented that she thought menopause was something that “just sort of happened”. “¯She shared, “I guess like when I got my period for the first time – it started without warning. So [I thought my periods] would just stop, and there would be much rejoicing.”
We followed up with the question of what surprised them most about menopause. And their answers were just as unique as the experience of menopause is to every woman. While the majority of respondents answered that they suffered with multiple vexing symptoms, we were delighted to hear it wasn’t all bad. Some women are also finding the silver lining in this transitional stage of life. As one woman put it, “Menopause isn’t just one thing, but many experiences. And it doesn’t have to mean that I’m old or past my prime. I can still feel good and vibrant and have energy. Weight gain isn’t inevitable and CAN be controlled. I can build endurance and strength if I carve out the time. And I’m worth the effort. That said, the inability to sleep soundly and consistently has been the hardest and most frustrating aspect of menopause.”
Women learn from other women’s experiences. And feeling like you are not alone in menopause can be very good for your emotional health. Here are 25 surprising things women shared they have experienced with menopause.
What has been the most surprising aspect of menopause?
- “How much the change in hormone levels affects every aspect of your life.”
- “How my body and brain are fairly unrecognizable when compared to my body and brain of even 12 months ago.”
- “Hair loss, sleeplessness, forgetfulness, belly fat (even though I never had children).”
- “Mood changes, joint pain, itchy & dry skin, scalp hair changes, breast cysts forming, vaginal dryness, digestion slowing down, that it can start many years before actually stopping!”
- “The most surprising aspect has been how hard menopause hit my body. I’ve always been blessed with good health and an active lifestyle. I never expected to develop vertigo, an anxiety disorder, or have my nervous system feel like it’s on fire. I never thought it would disrupt my life as it has. And I never thought I would fight with my body so much.”
- “I was most surprised that my OB/GYN really couldn’t help with this aspect of my health. Not a lot of knowledge about menopause and she did not have the time to review all the options out there for me to explore like HRT, supplements, and lifestyle changes.”
- “That I started perimenopause WAY, WAY before I even knew what was going on with my body. I had no idea why I felt the way I did, and why my periods were so terrible for so many years in my early 40’s. How tired I would feel. How it would affect so much of who I am; my confidence, my sex drive, my energy level, and don’t get me started with the brain fog. So much brain fog. It’s scary.”
- “That it happened so early.. also Lichens sclerosis.”
- “I’m amazed that my sleep is now so compromised. I can fall asleep no problem, but staying asleep is a challenge.”
- “How it has affected my life as far as having brain fog, anxiety, ringing in my ears.”
- “That at a certain point you start experiencing a lot of different symptoms, some days more some days less, your body starts changing and your brain too…and you start asking yourself what’s going on? After a while you ask yourself why nobody told me about this?”
- “The feeling that my body has lost control of its normal disposition. I experienced extreme anxiety attacks, palpitations and an elevated heart-rate. Nothing I had heard of being the typical menopause symptoms”¦”
- “I get nauseous right before a hot flash.”¯ Also, how night sweats come one right after the other and I haven’t slept in weeks.”
- “Crawly skin, tingling and pins and needle.. heavy head/burning scalp/ and muscle weakness to name a few.”
- “To lose my eyebrows”¦ and grow facial hair on my lip and at the side of my face.”
- “Neurological symptoms: brain fog, mood swings, depression.”
- “It totally sucks! I hate not feeling in control of my moods or my body!”
- “My biggest problems were the symptoms I did not attribute to menopause.”¯ I was deeply concerned I was in early onset Alzheimer’s.”¯Unable to find words, not complex words but everyday nouns.”¯Both of my Grandmas had Alzheimer’s, but not at the age of 50.”¯ The utter relief I felt after learning this happens in menopause, I can’t even describe how I felt!”
- “Anxiety. Major mood swings. Emotional rollercoaster. No libido.”
- “How fast it has hit me. And the amount of discomfort I have in my feet and legs on a daily basis”
- “Loss of words, hairs in new and unwelcome places, the sudden onslaught of anxiety over unfixable past actions, social anxiety, and the sharp increase in caring what others think of me.”
- “How absolutely out of control I feel. I have been suffering from such random symptoms like rashes, headaches,”¯ heavy periods, joint pain, anxiety,”¯ depression, weight gain. I thought I was going mad! I am 48 and I feel like an old woman. A few months later, I realized that I was in real trouble when I started feeling anxious and depressed. Please note that I have never ever suffered with either.”
- “I LOVE being the AGE of menopause.”¯ I wish I had more answers so I could move through it with more clarity.”¯ I’d love to feel like I had more control.”
- “The increase in confidence in who I am and what I have to offer, and I pick things and activities because I like them, not because of how others will perceive me.”
- “The freedom and empowerment.”
Your menopause journey is as unique as you are. And while some symptoms are more common than others, our integrated menopause care team is trained to support you through them all. Join the 94% of women who have found relief in menopause by visiting with a Gennev board-certified OB/GYN who specializes in menopause.
“
The information on the Gennev site is never meant to replace the care of a qualified medical professional. Hormonal shifts throughout menopause can prompt a lot of changes in your body, and simply assuming something is “just menopause” can leave you vulnerable to other possible causes. Always consult with your physician or schedule an appointment with one of Gennev’s telemedicine doctors before beginning any new treatment or therapy.
“
Weighing the benefits and risks of hormone replacement therapy (HRT) related to menopause can be one of the most confusing decisions a woman will make over the age of 50. There is no one-size-fits-all recommendation that can make the choice simple, or standardized chart to reference “if this, then that” scenarios. Every decision about HRT should be individual, and best when made between a patient and her health care provider.
Additionally, the care and treatment of menopausal women is complicated by the varied level of training and specialized experience of health care providers related to menopause. Not all OB/GYN’s or other health care providers have studied the latest research related to the potential benefits and risks of HRT in accordance with personal and family health history – research that increasingly demonstrates a window of time where HRT can provide both symptom relief and, in some cases, delay or ward off disease.
Most problematic is the legacy effect of how providers understand and interpret the seminal research that has been the basis for standardized care for HRT”a study completed two decades ago”called the Women’s Health Initiative (WHI). The 2002 study was conducted with women at an average age of 64- 65, and cited health risks associated with HRT around cancer, blood clots, and heart disease. Many healthcare providers have not kept up with subsequent publications on this data that showed that in women who were younger when they started, the risks are fewer and benefits greater. This has come at a cost to menopausal women suffering from sleepless nights, brain fog, painful sex, and hot flashes.
Thankfully, attitudes are shifting as new research surfaces. Both the Endocrine Society and the North American Menopause Society state that for symptom relief, the benefits of FDA-approved hormone therapy outweigh the risks in women younger than 60 or within 10 years of their last period, absent health issues such as a high risk of breast cancer or heart disease. The menopause society position statement adds that there are also benefits of HRT for women at high risk of bone loss or fracture.
With a bit of education, and having an informed conversation with a doctor, OB/GYN, or a menopause specialist, women are moving beyond the decades-old stigma of the HRT health concerns. They are creating personalized preparedness plans with their doctors as to when hormone therapy, if used as directed, might deliver more benefits than risks.
3 questions to ask your doctor about HRT
To evaluate with your doctor whether hormone therapy could be right for you, at what age, for how long, and what type, see the below set of questions and considerations to review in advance of your appointment, or to guide conversations with your doctor.
Based on the severity of how my menopause symptoms are impacting my quality of life and daily routine, would HRT potentially deliver relief?
- There are 40+ symptoms associated with menopause. The most common include hot flashes, vaginal dryness, painful sex, insomnia, fatigue, headaches, joint pain, anxiety, mood swings, memory lapses, digestive problems, and brittle nails.
- It is up to each individual woman to decide when and how her symptoms are impacting her quality of life and need addressing to provide relief.
- As some of the above symptoms can be related to other health issues, it is helpful to discuss which tests and screenings could be done to rule out other health concerns.
How might my health history, and that of my family, such as heart disease, strokes, dementia, osteoporosis, etc. factor into the benefits or risks of HRT?
- HRT may be especially beneficial if you have a family history of”¯osteoporosis, high”¯cholesterol, and”¯heart disease. On the other hand, it may not be best if you have”¯gynecologic cancer,”¯ or a blood clotting disorder.
- There is increasing evidence that starting HRT at the transition to Menopause can reduce the risk of Alzheimer’s, as discovered in studies by Dr. Lisa Mosconi.
- Research on cardiovascular health shows increasing evidence that starting HRT in the early years of menopause can provide cardiovascular benefit with reduced risk of cardiovascular disease. This benefit changes with age, and HRT may become riskier as you get further into menopause.
- There is evidence that HRT can help prevent osteoporosis.
- If you still have a uterus, Progesterone is recommended along with Estrogen to avoid the risk of uterine cancer. However, progesterone does slightly impact the incidence of breast cancer. The increase in risk is actually very low.
- If you have a family history of breast cancer, hormone therapy will not impact your risk (which is based on family history and genetics), and may be a valid choice for you.
Given my symptoms and family history, why type of HRT is best and for how long?
- Some of the options for HRT include topical, vaginal, oral pills, and patches”all with pros and cons and are described here.
- FDA regulated forms are always safest, and your doctor should be recommending these.
- Length of use of HRT is based on your symptoms and benefits from HRT, and varies woman to woman. There is no set stop date or number of years after which you must stop.
As research continues to emerge that demonstrates the benefits of hormone therapy for short term symptom relief and long-term risks related to heart, bone, and brain disease, there is no doubt decision making will become easier and standards will shift. Until that time, women at the age of 45 can have a conversation with a Gennev OB/GYN or their physician about how HRT might be considered as they move through menopause, and under what scenarios. This can set a valuable benchmark to inform treatment, if needed, in line with their own personal and family health history, and their individual health goals.
“
The information on the Gennev site is never meant to replace the care of a qualified medical professional. Hormonal shifts throughout menopause can prompt a lot of changes in your body, and simply assuming something is “just menopause” can leave you vulnerable to other possible causes. Always consult with your physician or schedule an appointment with one of Gennev’s telemedicine doctors before beginning any new treatment or therapy.
“
With all of the knowledge, self-awareness, and confidence that we gain as we age “about ourselves, our bodies, our turn ons and turn offs “ sex after 50 can be some the best sex of our lives. I know that can be hard to believe. We’ve all heard the negative messaging around menopause as the period of time when we lose our libido as well as our physical ability to enjoy sex. As a physical therapist who helps patients maintain their pelvic health, at every stage of life, I can tell you that it doesn’t have to be true for you.
Yes, menopause brings about significant changes as your ovaries stop producing estrogen. But, by focusing on your pelvic health, you can not only prevent and improve pelvic floor issues that put a damper on sex, you can also connect with your body in new and pleasurable ways.
Low Estrogen & Sexual Functioning
Several menopause-related changes can impact the way your body feels and functions during sex. As estrogen levels decrease, blood flow to the tissues of the vulva decreases, which can affect the size of the clitoris and its sensitivity to stimulation. The tissue of the vagina can become thinner and less flexible, and you may produce less natural lubrication which can lead to pain during sex. The same dryness that affects the tissues of the vagina can also affect the tissues in your mouth, which can make oral sex and even kissing a challenge.
These changes also tend to coincide with age-related muscle and sensory shifts, which can pose even more challenges to maintaining and enhancing one’s sex life. For many people, weakness in the muscles that surround the vagina, bladder and bowel can lead to urinary leakage, constipation, sexual dysfunction and pelvic organ prolapse. All of these things can contribute to how we feel about, and how we experience sex.
But changes in your body are nothing new. Through every menstrual cycle since puberty, your body has changed. If you were ever pregnant, your body has changed. If you’ve dealt with major illnesses or injuries, your body has changed. This is not to say that going through menopause is easy or to minimize the impact that these changes can have on your life, but you’ve experienced major physical changes before “ and both you and your body are incredibly resilient.
There’s clear evidence showing that addressing pelvic floor muscle function, in conjunction with improving overall muscle strength and physical wellbeing, can help to reduce and even prevent many of these symptoms related to menopause. Which brings me to the power of your pelvic floor.
Tap into the Power of Your Pelvic Floor
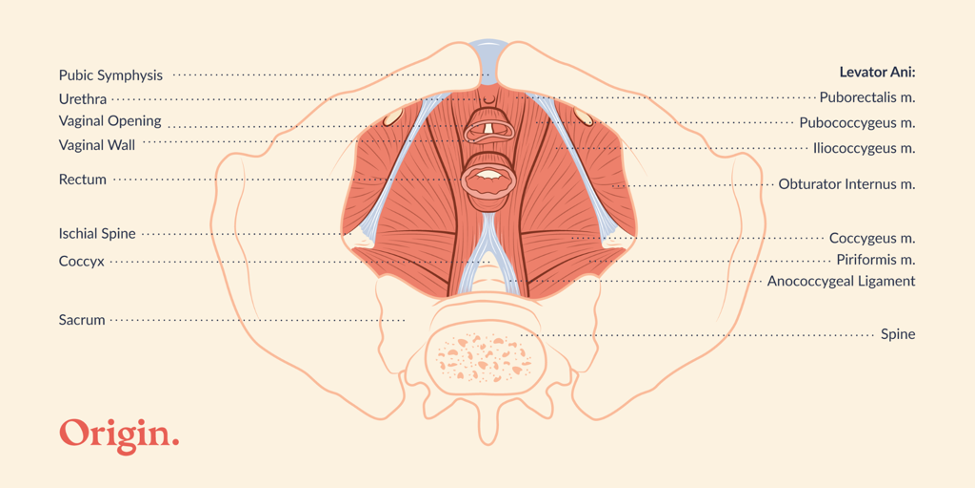
The pelvic floor refers to the multi-tasking group of muscles and connective tissues that make up the bottom of the pelvis. These muscles run from your pubic bone to your tailbone and wrap around the vaginal and anal openings. They also support and bring blood flow to the clitoris, vulva, and vaginal walls; and they are critical to maintaining and elevating your sexual function!
It’s important to keep all of your muscles strong and healthy as we age, and the pelvic floor muscles are no exception. During penetrative sex, the muscles that wrap around the anal and vaginal entrances, lengthen and open for pain free penetration and stretch, but they can also be squeezed for increased friction and sensation. Your pelvic floor is also important in orgasm with research showing that, during orgasm, the pelvic floor muscles will actually contract involuntarily.
Strong, healthy muscles have better blood flow, and during arousal, your pelvic floor helps to prepare your genitals for sex by bringing blood flow into your tissues, helping with tissue engorgement, and increasing nervous system activity and sensitivity in all of your pelvic erogenous zones (your clitoris, labia, vagina, anus, cervix, and lower abdominals for example).
This is why one of the most physically important things you can do for your sex life is maintain your pelvic floor health. If you are unsure of where to start, try these tips below.
Make sex a habit. The “use it or lose it” principle is particularly important after menopause. While it’s not uncommon for sex frequency to slow down, it’s important to consider that if you aren’t having sex, or if it’s less frequent, the vagina may begin to narrow with less flexibility and increased atrophy of the tissues, which can lead to more pain and dysfunction during penetrative intercourse. If partnered sex isn’t an option or isn’t something that interests you, this is a great time for solo sex. Masturbation with a penetrative sex toy can be a great way to encourage blood flow to your vulvovaginal tissues.
Explore different kinds of touch. You may also choose to focus on outercourse, if your vaginal tissues feel pain during penetration. As your nervous system, and tissues of the pelvic floor change, what may have felt pleasurable before could start to feel irritating and unwanted. By focusing on touch and sexual activity that is pain free and pleasurable for you now, you can avoid taking part in the pain cycle that so commonly surfaces in menopause. Consider reaching out to a sex counselor, if you are looking for further guidance on how to explore different kinds of sex.
Maximize your pelvic floor muscle health. Even as we age, research shows that people who are sexually active and able to achieve orgasm tend to have healthier pelvic floor muscles. Since healthy pelvic floor muscles can encourage blood flow to where you need it most, you may consider learning strategies to improve your pelvic floor health, such as strengthening your pelvic floor or increasing the pain free flexibility of those muscles by using dilators or beginning a stretching program to address overactive and irritable muscles. It may even mean working on your ability to properly coordinate these muscles during sex.
To learn more about your pelvic floor and how it can improve your sex life, ask your gynecologist or primary care physician for a referral to a pelvic floor physical therapist. Your therapist will evaluate your pelvic floor muscle functioning and create a personalized treatment plan to address and prevent symptoms “ and help you feel good in your body right now, which may be the biggest sexual turn on of all.
Celestine Compton, PT, DPT is a doctor of physical therapy at Origin with a board-certified specialization in women’s and pelvic health. She continues to expand her knowledge and capabilities within the field of women’s health PT to provide her patients and community with the best care, advocate for her profession on local and national levels, and support the advancement of women’s health through contributions to research, public awareness, and education. As part of the Origin team, she hopes to do her part to raise the standard of care that all women receive at every stage of life and to improve patient access to quality care so that no individual, regardless of location, race, identity, education, sexuality, or economic status is left behind.
The information on the Gennev site is never meant to replace the care of a qualified medical professional. Hormonal shifts throughout menopause can prompt a lot of changes in your body, and simply assuming something is “just menopause” can leave you vulnerable to other possible causes. Always consult with your physician or schedule an appointment with one of Gennev’s telemedicine doctors before beginning any new treatment or therapy.
“
“
Menopause information and advice is available everywhere now, and literally at your fingertips. And with a quick search with Doctor Google, you could either find some very valuable resources, or be taken down a path of misinformation. Gaining reliable advice as well as evidence-based treatments to manage your symptoms is what we are all about here at Gennev. So, we tapped into Dr. Lisa Savage, board-certified OB/GYN, to answer questions from our community about menopause, and help dispel the myths and share the facts surrounding symptoms and treatments.
Will my migraines disappear after menopause?
Headaches are very common, and what happens during menopause is highly variable. I’ve had plenty of patients whose migraine headaches do get better, others who got worse and many who stayed exactly the same. It’s not predictable and it’s very individual.
Some women have a cyclic component to their headaches (menstrual headaches) that come on as a prelude to menstruation, and lift after your period is over. Those types of cyclic headaches generally get better with menopause when cyclic hormones are not playing a role. Ultimately, I think it probably takes about a year after that last menstrual period to really know where your headaches have ended up – and even after that, there may be some change that can go either way.
How long does it take to feel better on HRT?
Time to symptom relief is a really gratifying part of starting HRT because it doesn’t take long. It’s not delayed gratification. I always tell my patients I don’t want to overpromise, but typically results can be seen anywhere from 48 hours to a couple of weeks.
How long can you take HRT?
It’s very individualized, and it depends on how old you are, when you need to start, and how long you want to take it. HRT does not need to be a long-term commitment if you don’t want it to be. Some women will take it for a few years to relieve the worst of the symptoms, and some women will need it longer, especially if they started their menopause transition at a younger age. Usually when a woman is approaching 60, I’m looking to see if we can get her off HRT, assuming she was around average age for menopause”¦meaning she’s been on it for around 10 years. I like to describe the therapy goal as extracting the most benefit while minimizing risk. But again, it’s not written in stone and there’s no hard and fast stopping point. Some women have ongoing symptoms for which they need the HRT. The most recent NAMS statement on HRT has taken away some of the boundaries about duration of treatment, which allows for our favorite way to prescribe medication; that is, with a lot of individualization.
Should I fear using HRT because it can cause breast cancer?
The short answer is no, but the better answer is “it depends.” There’s no doubt that some susceptible women, such as those with certain family history or genetic risk factors, may not be able to or want to take HRT because it may fertilize a propensity to develop breast cancer. It’s true that with longer term use from combined (that is estrogen and progesterone”¦not estrogen alone) HRT, there’s a small increased incidence of breast cancer. It’s about 8 extra cases per 10,000 women, so the absolute risk is very low. The increased risk from two glasses of wine per night or eating red meat is higher, to put it in perspective. You do have to commit to screening mammograms and knowing your body. I put this in terms of risk benefit ratio more than cause and effect. So often the benefits are going to outweigh any potential risk. We consider the individual patient and her individual profile when it comes to HRT.
Can women start having migraines in perimenopause if they’ve never had them before?
I’ve seen women start having migraines in perimenopause, but headaches are so multifactorial, especially vascular headaches. And my sense is that the sleep disturbance that comes along with perimenopause transition may play a big role in headaches. We all know if we’ve had a restless night’s sleep, the next day we don’t feel as well in our body. Maybe more headachy. I believe there’s a real sleep disturbance component to these headaches.
If you are post-hysterectomy, do you need to take the progesterone with the estrogen?
The only job of the progesterone in HRT is to protect the uterus from overgrowth of the lining. So, if a woman does not have a uterus, whether or not she still has ovaries, then she doesn’t need a progesterone. There’s some evidence to show that the combination of the estrogen plus the progesterone (the E + P) is what can cause some additional risk over time.
Is there a connection between autoimmune diseases and menopause?
Autoimmune is highly prevalent in women compared to men, and estrogen plays a role in autoimmune disorders and immunity in general. But immunity is also influenced by genetics, lifestyle and environment, so it’s hard to carve out just the estrogen component. It definitely plays a role in some autoimmune disorders such as rheumatoid arthritis and MS as as they may get worse with menopause. Lupus sufferers may actually feel better with menopause. But this varies greatly as it’s based upon the individual patient.
Is it true that the earlier a woman starts puberty, the earlier they’ll start menopause?
Not necessarily. A lot of women think if they were a late bloomer, they will not go through menopause until later. Or perhaps they started their periods when they were ten years old, and think they’re going to finish earlier. These things are not necessarily correlated. The average age of menopause across the board is 51. The normal age range is 45 to 55, and it’s independent of how old a woman was when she started puberty. Family history may actually be helpful; that is, knowing how old your mother or older sisters were at the time of menopause may be somewhat predictive.
Should I worry if I’m 59 and haven’t hit menopause yet?
This is definitely older than average (by the age of 55, 95% of women have completed the menopause transition), but as long as you’ve been getting medical care from a clinician who is familiar with these things and there is good confidence based on menstrual history and (in this case) labwork, that you are still pre-menopausal and not having post-menopausal bleeding, there are benefits to ongoing ovarian hormone production. There is a silver lining there for your bones, cognition and cardiac health.
Is weight gain a side effect of HRT?
No, HRT does not cause weight gain. But it is true that many women start HRT coincident with the onset of menopause, which does bring metabolic changes. Increased weight around your midsection is very common at this stage of life, even if you have never had it before. It’s the body’s way of compensating for the loss of ovarian estrogen production, since estrogen can also be made in fat. To a certain point (say 5-10 pounds), I usually encourage patients to be accepting of a new normal and not too go crazy trying to maintain a weight that they were five or ten years ago. Some changes in nutrition can be helpful, along with getting adequate sleep, and exercise.
What can I do about hair loss or hair thinning with menopause?
It is true that aging in both men and women can cause hair to thin. I never automatically attribute this to menopause and always encourage patients to see their dermatologist. Thyroid disorders, among a list of other things, can cause hair loss. Depending on the pattern of hair loss on a physical exam, labs and/or scalp biopsy might be indicated. Menopause absolutely can contribute to hair changes, but please see your dermatologist for an examination, blood work and investigation before assuming it’s strictly based on menopause.
Does HRT prolong menopause?
HRT does not extend or prolong menopause. This is a common concern among women considering HRT. Menopause symptoms tend to dissipate over time naturally, and so your symptoms are going to be what they are at that age, whether or not you took any HRT.
Is there a certain age that someone is going to start menopause?
It’s highly variable. I always say 45 to 55, but a lot of women will start to notice changes in their late 30s and I call those prelude symptoms. This is when symptoms tend to come and go. Certainly, into your mid 40s it is very common to start seeing some symptoms, even if they’re not consistent.
Is a woman infertile because her periods have become irregular?
You may still ovulate from time to time until you have gone a year without a period. So even if your period is not regular and predictable, I always tell my patients they still need contraception until they’ve been a year without a period. Irregular periods are not a form of birth control.
Is more painful ovulation a sign or symptom of perimenopause?
It doesn’t seem fair that when we’re trying to end our reproductive years that we have to get more pain with it. But I’ve seen many patients that report more painful ovulation and periods, and more PMS during perimenopause compared with the earlier years of their reproductive life.
If my hormone labs are normal then I’m not in menopause or perimenopause, right?
Not necessarily. Labs indicate levels in a snapshot – a moment in time as and they may vary a lot from one day to the next. If we look at a woman at the right age with classic symptoms, the labs might still be normal, or they may be normal today and not tomorrow. So, it’s good to not to rely on them, as normal labs may not mean that it’s not perimenopause.
What are your tips for relieving increased PMS during perimenopause?
There are a lot of holistic things I go back to like exercise, eating well, and adequate sleep. I have prescribed very low dose birth control pills for women in perimenopause who have a lot of PMS as women who do not ovulate do not have a lot of PMS symptoms. The pill eliminates ovulation so that that can be a nice transitional thing to do.
How do you feel about testosterone pellets as hormone treatment?
I don’t use them. Testosterone is typically prescribed for libido, and in order to make a difference on that, you have to use really high doses of testosterone. I call that trying to make a woman into a man – and there may be some cardiac risk associated with that. So, I am not a believer in the use of testosterone for women. Other doctors disagree, and I respect that, but I’m not a fan of testosterone in any form, whether it’s pellets or creams, patches, etc., and I’ve not found it to be helpful.
If you are in menopause, should you avoid regular Pap smears or have them more frequently?
Menopause really doesn’t influence our Pap recommendations for most women over the age of about 30. If you’ve had normal Paps, you can get one about every third annual. There are some age-based recommendations on how often to get a Pap, but typically we’re going to do Paps up to the age of about 65, assuming normal results over time. Menopause doesn’t influence whether or not to get a Pap smear.
Will all this extra protein in my diet make me fat?
I always promote a diet consisting of lean protein and vegetables, more specifically the Mediterranean way of eating. I think we really have to watch out for the carbs and especially refined sugars. As we age, we’re losing muscle, and estrogen does play a role in maintaining lean muscle mass. So, when your estrogen is decreasing and your muscle mass is naturally decreasing, having that additional protein can help to rebuild, repair, and maintain that muscle.
Are low dose antidepressants effective for hot flashes?
Yes, I’ve had some good luck with this. Especially for patients who cannot take hormone replacement therapy, or don’t want to. We know that certain low dose antidepressants can help with hot flashes. Additionally, menopause frequently brings mood disorders. It can unmask depression and anxiety or make it worse. So, you may get some double coverage by using a low dose antidepressant for hot flashes and moods. But I will say that as helpful as they may be, there’s nothing as effective as estrogen for relieving hot flashes.
What is your trusted advice for women going through menopause?
I always say be aware of “Doctor Google”. Getting your information from Doctor Google can be like drinking out of a firehose and you don’t know what’s reliable and what’s not. Rely on your physician, and specifically in menopause, your OB/GYN physician. Narrow your resources to reliable ones such as gennev.com, acog.org and menopause.org.
You can listen to the “Menopause Myths & Facts” interview with Dr. Savage here.
We can help relieve your menopause symptoms
You deserve the support, education and specialized menopause care that will help you start feeling better now. Learn more about Gennev’s Integrated Menopause Care by clicking here.
“
The information on the Gennev site is never meant to replace the care of a qualified medical professional. Hormonal shifts throughout menopause can prompt a lot of changes in your body, and simply assuming something is “just menopause” can leave you vulnerable to other possible causes. Always consult with your physician or schedule an appointment with one of Gennev’s telemedicine doctors before beginning any new treatment or therapy.