It is my honor to introduce the Click here“>changes to Gennev to support 38M women in menopause in the U.S!
Gennev began in 2016, and through its evolution became the first-ever online clinic for women in menopause with telehealth services, products, and education.

As any startup company knows, you build the technology from the ground up until you understand what consumers will use and if they will pay for your services.
Gennev has been on that journey. We have supported millions of women who have consumed our education, engaged 60,000 through the Gennev Menopause Assessment, and have provided telehealth services, memberships, and products to thousands who need quality health care.
Today we’re moving from our “starter” technology platform to the new Gennev as a more secure intelligent platform that is re-imagining the way women manage menopause help.
What changes is the technology that powers our menopause care for women: it now delivers an improved user experience, a more secure and flexible data architecture, and a platform for extreme growth. What doesn’t change is our mission to empower women to take control of their health in the second half of life”¦starting with menopause. Because we have millions of women yet to serve.
As a woman, a mom, and Gennev’s VP of Technology, I’m proud of what we’re delivering today. I’m excited about what it means for millions of women. I’m proud to be building a platform for myself, a 44-year-old woman who is pre-menopausal.
For women who care about quality healthcare, this article will share how we’re empowering you to take control of your health. For the technology and health care enthusiasts reading this article, I share my fundamentals for building customer-first digital health platforms for the masses during COVID-19 times. And for the nay-sayers who never thought digital health for menopause could be a viable business, we’re just getting started.
The Back Story
How do you build a platform for talking about something society doesn’t talk about?
When I came to Gennev a year ago, that was the task I was facing: reimagining and building a platform for one of the biggest remaining societal taboos. Menopause.
Gennev CEO Jill Angelo asked me to find a way to connect menopausal women to health care providers, products, education, and community through a safe, intelligent recommendation engine. Sort of like Amazon can forecast our consumption for products. Gennev wants to keep women in the know for what they will need throughout the menopause journey.
Because Gennev was an early start up, the telehealth and ecommerce platform built up to that point didn’t have the flexibility or the power to handle current needs, much less the exponential growth we were experiencing.
A history of technology and health care
Looking back, my work history has always been grounded in helping others.
As a young engineer, I started my career managing customer tech support at an internet-connectivity startup. Then came September 11, 2001; I was working in lower Manhattan. That traumatic experience really catalyzed my desire to use my career to improve the lives of others.
I was interested in health and health outcomes, so I went back to school for a Master’s in Public Health. I moved to Seattle because there were so many opportunities in public health. I merged my passions for computer science and public health when I landed a role at the Fred Hutch Cancer Research Center. I created a new online data sharing program for HIV vaccine trials.
Lesson One: Listen to the end user
I worked in the Vaccine and Infectious Disease division, then moved to Central IT to work on clinical data repositories for cancer researchers, including data visualization tools. Then my team started building an informatics department. None existed at Fred Hutch before, but we really wanted a way to accelerate research that utilized the cancer patient data.
It took a lot of interviewing researchers and medical providers to understand what they needed to get the right tools and data into their hands for their research. But I learned an exceptionally valuable lesson there, one that seems so easy but is so rarely employed: listen to the end user.
There was a lot to parse out. What did it mean to enable meaningful use of medical record data? How could we implement technology systems and stay within regulatory frameworks? How could we keep data safe, but still make it accessible; how could we comply with federal law and patient best interests, when sometimes they seemed at odds?
When data is siloed in a bunch of different places and systems that not only don’t connect, they often don’t speak the same language, bringing it together, making it useful, and keeping our own biases out of it is tricky business. But I learned some invaluable lessons there about how to respect the need for data security while meeting the need for useful access to that data.
After ten years in health care research, I was feeling disconnected from the patient experience. I couldn’t have as tangible an impact as I wanted if I didn’t understand the patients’ perspective. So I moved into consumer health care.
Lesson Two: Build Trust through Tech
I joined Providence Health Systems’ Digital Innovation Group, and that’s where I led the team that built the Circle mobile app for pregnant women and new moms.
The thinking behind the Circle app was there was a lot of information out there for pregnant women and new moms, but these women were really searching for a voice they could trust. Regular engagement with those women would build that trust, and when they needed to see a doctor, they’d come to us because they knew us already.
The app gave them information about how their baby was developing, what checkups they needed, what medication they should be taking, all the thousand-and-one details women have to keep straight. I was a new mom with two littles, so I could really understand the questions these women had, the concerns they had. I used trackers too “ diapers, sleeping patterns, vaccines “ but they were all on these separate apps, and I was too exhausted to make sense of them all. So when it came time to create an app, we brought them all together.
And that was another important lesson I brought with me to Gennev: you can build trust through technology, but only if your tech is built with the consumer’s experience in the forefront. You can build all the cool features you want, you can make it look beautiful, but if it doesn’t tell me that my belly is jumping because my baby has hiccups, it’s not useful to me.
Women make 80 percent of the health care decisions for their household. Men frequently are the ones who design that health care. It took Apple as in many ways the gold standard for UX/UI “ until iOS 9 to add period tracking to their HealthKit app. For women, it just wasn’t as useful. They had to download other apps or look to other devices to fill that need. It’s not that the male developers did it on purpose or didn’t think it was important, they just hadn’t seen their users as female.
When you foreground your user, you see things others don’t. When you reflect the user’s experience back at them, accurately and faithfully, that builds trust.
Ultimately Circle was acquired by Wildflower Health, where I got exposure to progressive, innovative thought around women’s healthcare. Through that experience, I learned how underserved women were beyond just the child-bearing years as particularly in menopause.
I met Jill, and my next step was set. Her passion for truly serving this underserved community of women who are often really struggling with symptoms, was impossible to resist. And knowing I could be in that boat one day made it even more compelling. Jill has built an amazing team of experts, and I was really excited to build them a first-class platform to take them to the next level.
Lesson Three: Build the team; leverage the moment
My mission is to reduce barriers to usability, both for consumers using an app and for researchers using the data from that app to create better solutions and outcomes.
That is especially important in this work for Gennev. Women 40+ have been ignored and dismissed for so long, the last thing they need when they finally find a resource to help them is more hurdles. My north star is to keep it simple. I don’t mean “dumb it down” as those things are often confused in this business, I think. I mean keep it simple. Light the path.
To do that, I recruited a team with a broad range of skills and perspectives.
Software development can no longer be done by a single coder: finding a designer that gets your end-user (in our case, the designer is a woman who went through menopause at an early age) is paramount. And finding a QA Engineer that gets how female consumers use technology is crazy important; finding the right men who don’t flinch at talk of hot flashes is rare, but we won the lottery on talent!
And in COVID times, finding the right talent who can work effectively from home, connected through tools like Slack and Zoom, has been paramount to delivering the new Gennev. My team has chemistry and a diverse set of backgrounds, which has been a huge asset in delivering our new platform.
The COVID crisis really sped up a lot of things that we were already doing. Healthcare has to come to the consumer. We were already working towards that with our telemedicine, but we were up against the barrier of people not really understanding how they could get adequate care via a video in their living room.
COVID sped that up by years, probably. Suddenly you didn’t have a choice, so you tried it. And lots of people found they could get what they need just fine.
We’ve effectively built a new kind of EMR for GenX women who want access to their data, appointment follow-ups, and recommendations. Our team of 25 OB/GYNs and 3 Registered Dietitians need a flexible way for personalizing care options as prescriptions, over-the-counter supplements, education, and community resources for their patients. The new Gennev accomplishes both. And it does so across 49 states for telehealth and all 50 states for our HealthFix Coaching Membership.
Lesson Four: Learn scrappy
One thing I’ve learned from the incubation lab at Providence Healthcare and now Gennev is “learn scrappy.” Find a way to do the tech-enabled thing you want to do in a small, non-technical, scrappy way so you can test it.
At Gennev, we’re building the first-ever intelligent menopause roadmap that recommends care options for women based on where they are in the journey. To do that, we need to have quality data and use it in such a way that the tech is getting more intelligent about forecasting and recommending what a woman needs before she knows it. And we have to be transparent with her about how we’re using her data to her benefit.
To get there, we’re applying quick experiments in non-tech-heavy ways using SMS, email and good ol’ fashion customer service. We’re learning, and every bit of that learning has gone into the new Gennev.
Lesson Five: Review customer feedback
Are we providing our customers and patients with information they can understand and act on?
One of the things I love most about Gennev is we walk the walk. When we say we’re here to help women, we mean it, and that starts with our technology. We want a system that allows women to tell us what they need.
Last week, we received this feedback from a HealthFix Coaching Member:
Customer feedback is a constant reminder of how important it is to be focused on them and what improves their quality of life. It sets the direction for our technology roadmap, and it is a guiding light (and affirmation) for business success.
Gennev has built the largest data set about women in menopause of any company in the world. We’re out to change women’s experience with menopause, to make it something to celebrate rather than dread. Technology powers this change. It’s not the hero, but with the new Gennev, we’re advancing how millions of women manage their menopause.
Do an Internet search on “soy, menopause,” and you’ll typically find a couple of schools of thought: soy is dangerous because the phytoestrogens in soy increase breast cancer risk. Or, soy helps relieve perimenopause and menopause symptoms thanks to those same phytoestrogens.
So, is soy dangerous?
No. Eating a moderate amount of whole-soy foods will not increase your risk of breast or any other kind of cancer, even if you’ve had breast cancer or have a family history of the disease.
Why do we think soy is dangerous?
Concerns about soy and a link to breast cancer date back to a study done in 1996 and published in Cancer Epidemiology, Biomarkers, & Prevention. The study seemed to indicate that soy protein could stimulate the growth of breast cancer cells.
Researchers had known prior to the study that isoflavones, an estrogen-like compound found in soy and may other foods, can mimic the natural estrogens of the body. And since higher estrogen levels can increase the risk of breast cancer, it followed that isoflavones could have the same effect.
However, Dr. Omer Kucuk, medical oncologist at Emory University’s Winship Cancer Institute, told CNN, there are two estrogen receptors in our bodies, alpha and beta. Binding to alpha receptors may increase the risk of breast cancer by making breast cells grow.
“Soy isoflavones bind preferentially to estrogen receptor beta,” says Dr. Kucuk, and may actually have a protective effect against breast cancer. Hence the lower cancer rates in high-soy-consumption parts of the world like Japan and China where people consume soy throughout their lives.
There may be negative effects for people with thyroid issues, especially in women. If you take medication for hypothyroidism, soy may interfere with your body’s ability to absorb that medication. However, says the Mayo Clinic, if you take your medication as prescribed and wait four hours after taking your medication before consuming soy, you can enjoy whole soy-based foods without concern.
What are the benefits of soy?
The jury is still out on many of the claims soy proponents have made through the years, but evidence that soy is genuinely good for us is piling up.
- Soy is rich in protein and contains a full complement of the nine essential amino acids.
- The isoflavones in soy may contain anticancer effects, including reducing the risk of recurrence in women who’ve already been diagnosed with breast cancer.
- Soy contains omega-3s, which may help protect our brains, and which many in the West don’t get enough of.
- The nutritional composition of soy (with saponins, omega3s, dietary fiber, etc.) may help prevent heart disease, diabetes and cardiovascular disease, as well as protecting against some types of cancer.
How can we safely consume soy?
While the experts still disagree on exactly the benefits and risks of soy, most agree that soy is best consumed as “whole” as possible.
Look for minimally processed versions such as edamame, tofu, tempeh, and miso. Avoid or limit highly processed vegetarian meat or cheese substitutes which can contain a whole lot of other stuff, negating the benefits of soy. Lots of protein bars contain soy, but the processing and the added sugars may make those foods less than healthy.
Additionally, soy or isoflavone supplements may not be a good way to enjoy the benefits of soy, as large-scale studies on soy supplements haven’t really been conducted to date, says Dr. Kucuk. In fact, says Katherine Zeratsky, RD LD, for the Mayo Clinic, some studies suggest the higher levels of isoflavones in supplements may actually increase the risk of breast cancer.
As with most nutrition, it’s best to meet your needs with real food: “25 grams a day” was the amount several nutrition experts gave as a guideline for safe consumption of soy, and “fermented” likely yields the highest nutritional value (natto, tempeh, miso).
Does soy help with menopause symptoms?
OK, so the phytoestrogen in soy won’t cause breast cancer, but will it end hot flashes?
Great question. Results, as with All Things Menopause, are mixed. Some studies seem to show that isoflavones reduce the severity and frequency of hot flashes as this study, unfortunately, centered on the use of soy supplements, which, as discussed above, aren’t ideal.
Another, earlier study found no evidence that plant-based estrogens like soy or red clover had any beneficial effect.
The protective and beneficial effects of soy may also depend on how long a woman has consumed it. Women who’ve eaten soy regularly over their whole lives seem to receive greater benefits than women who come to it later.
However, given the low-or-no risk and the very real health benefits of eating soy, why not try it? As ever, if you’re making a significant change to your diet, running it past your doctor is never a bad idea, especially if you’re on medication and have concerns about interactions. And if your morning miso soup results in fewer, less disruptive hot flashes, so much the better.
Do you eat soy? Why or why not? If you’re a soy lover, how about sharing some recipes with the rest of us? You can talk with us in the comments below, in our community forums (you’ll need to join our community first, if you haven’t already), on our Facebook page, or in Midlife & Menopause Solutions, our closed Facebook group.
If you are constantly feeling an upset stomach (gas, diarrhea, bloating, and heartburn), weight changes, constant fatigue or skin irritation, these can all be signs of an unhealthy gut. You should pay a visit to the bulk section to stock up on foods to eat for a healthy gut. The bulk section can be intimidating. I’m an avid cook, and sometimes even my head starts spinning when I head down the bulk aisle! There are so many choices, so many different varieties of grains, legumes, flours, etc. For cooks who are comfortable with food, it can be a treasure trove, but for the average person, it can be a challenge, and just knowing where to begin is quite overwhelming.
But don’t give up! If there are two aisles of the grocery store you should be frequenting, it’s the bulk aisle and the produce aisle. What I love about the bulk aisle is that it is bustling with nutrients! There isn’t any fancy packaging vying for your attention and your dollars as it’s food in its purest form (granted, there can be a few sugar-coated exceptions in the bulk aisles you should avoid).
And looking beyond nutrition, the bulk aisle is a great place for the budget conscious. You don’t need to buy in bulk, you can simply buy what you need.
Here in Seattle, we’re lucky to have PCC Markets, the largest consumer-owned natural food retail co-operative in the United States with eleven stores throughout the greater Seattle area. When you want great bulk-aisle selections, there’s no better place to go. Think Whole Foods on steroids!
I recently toured a local PCC with their resident nutritionist, Marilyn Walls, and asked her to weigh in on the top 10 foods to bulk up on in the bulk aisle. This list is sort of a “bulk foods starter kit” and was designed with your body and mind in mind.
How Do I Get A Healthier Gut?
Research shows there is a powerful connection between our gut health and our emotional well-being. By nourishing the gut with real, whole foods, vegetables, fruits and lean proteins, you can positively impact your mind and your body. Therefore, we’ve chosen a variety of bulk foods, from spices and grains, teas, seeds and legumes, all of which are nutrient-dense and rich in fiber, properties that can help with pesky menopause problems like bloating, digestion, and even memory loss.
Most grocery stores have a bulk aisle, so I encourage you to make a beeline for the bulk section on your next visit to the store and try some or all of the suggestions on this list. And remember, the beauty of bulking up on these whole foods is that they won’t weigh you down, but rather, will amp you up with all-natural goodness.
Cheers to your health!
Michelle
List Of Foods To Eat For A Healthy Gut
ItemBenefitsUses1TurmericContains curcumin, a substance with powerful anti-inflammatory and antioxidant propertiesAdd 1 teaspoon into tea, sprinkle onto eggs, into salads, onto rice, sauté with tofu.2Loose green teaHigh in anti-oxidants. Promotes heart health, brain health and helps with digestion.Substitute green tea for soda/coffee.3Forbidden black riceRich in antioxidants (evidenced by its color). Also filled with flavonoid phytonutrients, a good source of fiber, minerals and plant based protein. Gluten free.Serve as a side dish. Toss into a salad.4LentilsHigh in fiber, protein, folate, other minerals.As a salad or in salads, soups and in healthy dips. Click here for my recipe for lentil salad.5Adzuki beansGood source of magnesium, potassium, iron and other vitamins/minerals. Easy to digest.Use in soups, as a side dish. Popular mashed and sweetened and eaten as a treat in Japan.6Freshly ground almond butter (unsalted, no sugar added, freshly ground on site with only almonds)Great source of healthy fat, rich in protein, fiber, calcium and magnesium.Spread on apples, celery, whole grain toast/crackers. Use as a base for an Asian dressing. Limit serving size to 2 tablespoons.7Almonds (unsalted, unroasted are recommended. Sprouted and organic varieties have the most benefits.Packed with protein, fiber, antioxidants, vitamins and trace minerals.Eat as a snack, toss onto salads or rice dishes, use in a healthy pesto.8QuinoaRich in protein, a good source of riboflavin, gluten free and has a low glycemic index.Use in a bowl tossed with veggies, sprinkle onto salads, layer into a wrap sandwich.9Flax seeds (golden or brown)Full of fiber and omega-3 fatty acids.Add to smoothies, toss onto oatmeal, add to homemade healthy baked goods. Toast them and toss into a salad for an extra crunch.10Rolled or steel-cut oatsHigh in fiber, good for the heart in that it curbs LDL (bad cholesterol)Cook oats in a little water or your choice of milk, top with healthy ingredients.
Many thanks to PCC for lending us Marilyn Walls and letting us tour one of their markets!
About Marilyn Walls, PCC Nutrition Educator: Marilyn has a Masters in Nutrition from Bastyr University, and she has taught nutrition and herbs there for three years. During her ten years at PCC, she’s taught classes to customers, staff and lots of kids. She also writes articles for the PCC Sound Consumer newspaper. Having counseled many (sometimes crying) women, she believes menopausal symptoms may be alleviated through improved diet and herbal choices.
Last week we discussed why women often don’t get diagnosed and treated for a heart attack quickly enough. In brief,
- Culturally, we still associate heart attacks with men, so we’re slower to understand and respond when a woman is having one.
- Women’s heart attack symptoms differ from men’s and so are frequently misdiagnosed or ignored.
- Women may not demand treatment soon enough or loudly enough.
- And treatments are largely designed for men’s bodies and may not be appropriate for women.
Educating yourself on the symptoms of heart attack in men and women could mean saving a life as including your own.
But what’s even better than knowing what a heart attack looks and feels like? Never knowing what a heart attack looks and feels like.
Healthier Heart Tip 1: Nutrition
We all know the drill: more leafy greens, cut back on refined sugar, aim for quality, whole-grain carbs, reduce the meats, and boost the nuts, fruits, and veggies. But women’s bodies change during menopause, meaning their nutritional needs change too. Even if you’re not at high risk for heart disease, some dietary adjustments can help you meet your nutritional needs. Here are some special steps women can take to help preserve heart health:
- Phytoestrogens. Soy-based foods like tofu, tempeh, and soy milk can mimic the protective behavior of estrogen in supporting HDL cholesterol (the good kind). Additionally, many women report relief from menopause symptoms such as hot flashes and night sweats, and this increase in quality of life is good for your heart as well.
- Saturated fats. After menopause, LDL (bad) cholesterol may rise, so reduce or avoid foods high in saturated fats (red meats, whole-fat dairy products, some vegetable oils).
- Vitamin D and calcium. While not directly related to heart health, having strong bones makes it a whole lot easier to get the exercise that does help your heart. The jury is still out on how much more Vitamin D and calcium menopausal women need and the best ways to get it, but eating a spinach salad in the sunshine sounds like a plan.
Healthier Heart Tip 2: Exercise
Yep, finding the time and will to exercise is tough, but there are so many massive benefits to women over 40, it’s difficult to overstate the case.
- Avoid weight gain. As estrogen levels decline, weight often increases. And worse, it generally collects around the middle as and belly fat is a higher heart risk than fat on the hips, thighs, or backside. Increasing activity level (particularly while improving diet, re: Tip 1) can help you maintain a healthy weight.
- Improve sleep. Many women report interrupted (or frankly, really crappy) sleep during this phase of life, and that can be hard on your heart. Exercising regularly is a great way to improve sleep, but one word of caution: some women report exercising too close to bed time increases the likelihood of night sweats.
- Reduce anxiety and depression. Regular exercise has therapeutic effects on many people suffering from anxiety and depression, including women in menopause. Anxiety and depression can stress your heart; reduce them for a healthier heart and a happier you.
To maximize health benefit, it’s great to do a lot of things: a little weight-bearing, impact exercise for bone density (like running); strength training to build and maintain muscle (I love rock climbing, my friend Anne swings kettle balls); some good cardio-vascular for your heart and lungs (walking, cycling, swimming); and some focusing activity for strength of body and mind (yoga).
Whatever you do, in whatever combination, try to get in 30 minutes of exercise 5 days a week. Just be sure any increases are made slowly and carefully, so your body is ready for the demand.
Healthier Heart Tip 3: Lifestyle choices
Healthy diet and regular exercise are obvious ways to increase heart health and lower your risk of heart disease. But certain lifestyle choices can have huge heart-health impacts. Two of the biggies: smoking and depression.
Smoking. The 1950s called and they want their bad habit back. OK, we know it’s so much easier to say “quit” than it is to do it, but if you’re at or approaching menopause, now more than ever, you need to snuff out your last cigarette. Women who smoke may enter menopause sooner (meaning fewer years with estrogen’s protective benefits) and can experience more intense symptoms. Quitting smoking can be one of the most profound things you do to protect your future health.
Depression. A 10-year study conducted by Reading Hospital ob/gyn Xuezhi Jiang, MD and colleagues revealed that depression can contribute as significantly as to a woman’s risk of coronary artery disease (CAD) in midlife. According to Dr. Jiang, “We saw a significant difference in the association of depression with the risk for CAD based on a patient’s age. Compared with women aged 65 years and older, women under the age of 65 were far more likely to incur CAD as a result of depression.” Dr. Jiang strongly recommends that any woman at or approaching menopausal age who has a history of depression be proactive and get regular screenings.
Even if your feelings of depression don’t require professional intervention or treatment, all women can benefit from being proactive with their mental health. A big one? Staying social. Because of incontinence, hot flashes, and other “embarrassing” symptoms, women may limit social interaction during this time. Chances are other women in your age group are experiencing similar issues, so get together, talk it out, share solutions, and create the support network that can help you all be healthier.
Quoted or consulted sources:
http://www.health.harvard.edu/heart-health/11-foods-that-lower-cholesterol
http://www.medscape.com/viewarticle/737143_2
http://www.mayoclinic.org/healthy-lifestyle/womens-health/in-depth/belly-fat/art-20045809
http://www.healthline.com/health/menopause/sleep-problems#2
http://www.endocrinologyadvisor.com/nams-2016/cad-risk-and-depression-in-women/article/527431/
http://www.acsm.org/public-information/articles/2016/10/07/exercise-recommendations-for-menopause-aged-women
Menopause health concerns of fatigue , mood changes, and sleep disturbances lead the list of challenges with alarming impact on quality of life, but 94 percent of women don’t get enough support to manage side effects. Gennev, a first-of-its-kind online menopause clinic for women, today announced the first annual Menopause Zeitgeist, the largest survey of its kind with results from more than 6,000 women. The Menopause Zeitgeist captures the top perimenopause and post-menopause symptoms women faced in 2019 “ and what women want in 2020.

Introducing Zeitgeist Menopause Statistics
Although menopause is about as universal a condition as we can imagine (everyone born with a uterus goes through it, if they live long enough), the experience of menopause is as individual as the person going through it.
The amount of time the transition takes can range from months to years. Symptoms run the gamut from non-existent to life-altering. Some get amazing support from knowledgeable professionals. Some suffer alone, not sure what’s going on or how to manage the challenges.
And because our society still largely regards menopause as some sort of shameful secret, many of us feel like we’re out here on our own.
That’s changing. Wow, is it changing.
Modern menopause
Women are speaking up and speaking out, unwilling to let perimenopause and menopause derail their careers, dreams, relationships, health, or quality of life anymore. With women like Jennifer Aniston, Jennifer Lopez, and Gwen Stefani showing what 50 can look like, 2019 has been a celebration of women in midlife and a demonstration of what life can truly be on the far side of the menopause divide.
Menopause is now a topic of discussion on mainstream media as well as the subject of popular books such as Darcey Steinke’s Flash Count Diary, and getting “ at last! “ researched by scientists like Dr. Lisa Mosconi.
At Gennev, we’re loving being at the center of this new and swelling menopause zeitgeist, connecting women with the health care experts, products, and services that can help them feel great, and helping women connect with each other and find strength in a menopause group.
What is the new zeitgeist?
Books, talk shows, and cultural conversations aside, what matters is how the women in the thick of it are feeling about their experience. At Gennev, we recently conducted a survey of more than 6,000 women, asking about their menopause symptoms and the impacts those symptoms have on their lives.
Know your body better: learn your menopause type by taking our OB/GYN-designed Menopause Assessment
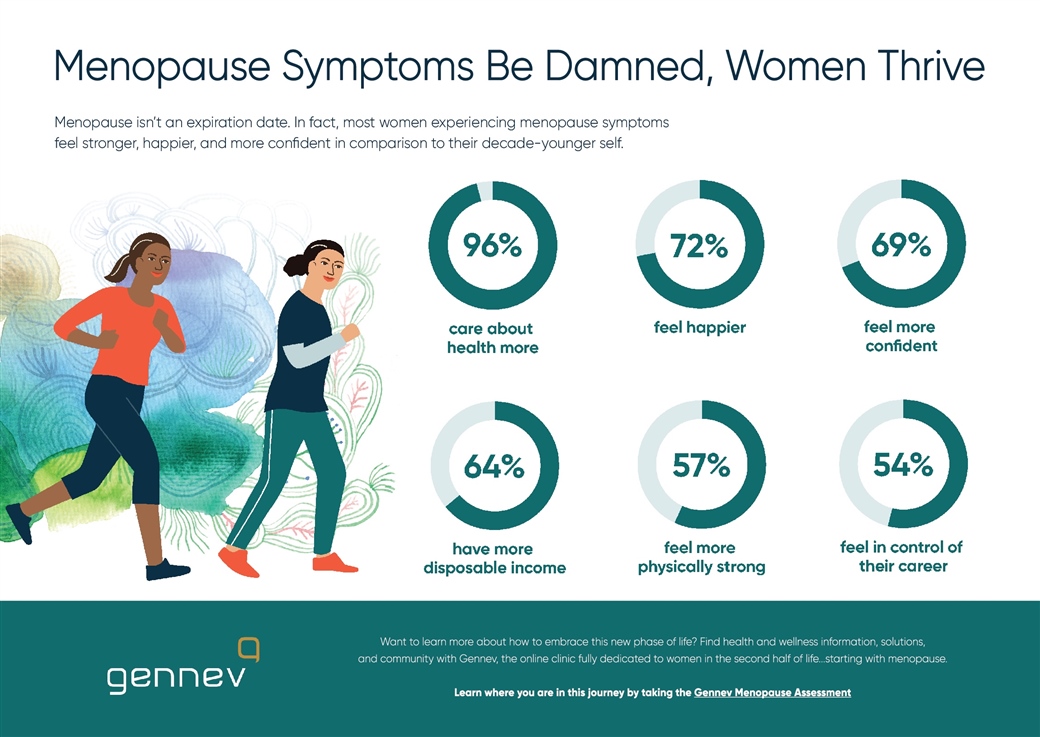
Women in menopause are thriving
This new spirit of the age reflects a new confidence. The good news is women are thriving through and beyond the transition: We’re feeling happier (72 percent), physically stronger (57 percent), more confident (69 percent), and more in control of our careers (54 percent) now than we did when we were 10 years younger.
But we could use more support
Where there’s “room for improvement”? There are some pretty important gaps that need to be addressed. Mainly, women are getting through this on their own, and any “thriving” that’s happening is happening in spite of menopause, not in harmony with it.
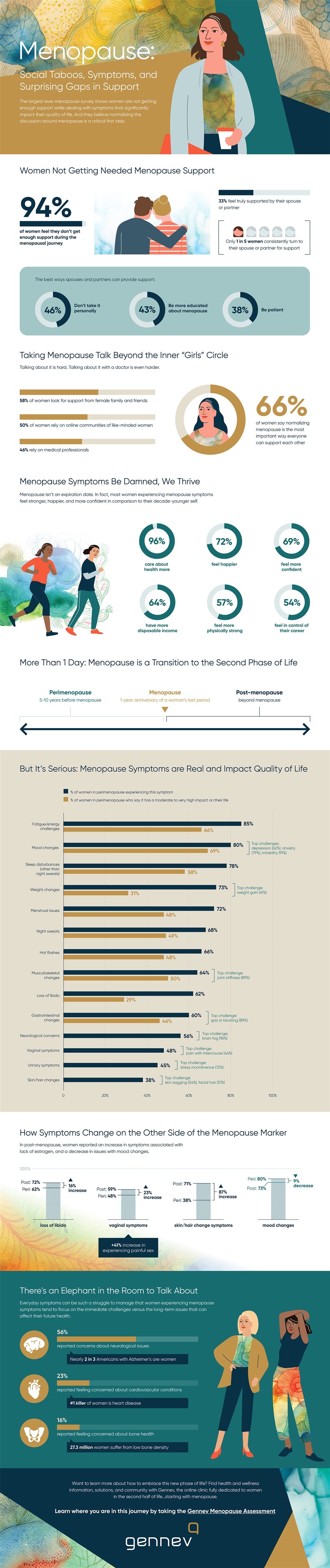
The biggest issue? We’re still not getting the support we need. Only 33 percent of the women we surveyed felt fully supported by their partners, and more than half (54 percent) felt undersupported by medical professionals. If you can’t turn to your doctor or partner for help as or even just to be heard as menopause becomes a much harder journey than it needs to be.
“Menopause is natural and normal, but a woman can almost feel like she’s going crazy when doctors or those close to them are dismissive of midlife complaints, of their pain, or are not well-informed about menopause,” said Dr. Rebecca Dunsmoor-Su, OB/GYN, North American Menopause Society (NAMS)-certified practitioner, and Chief Medical Officer at Gennev. “We want women and all those who support them to feel more prepared for this life stage, and make sure they have someone and somewhere they can go to understand what’s happening with their bodies and to feel supported.”
We need support and solutions for women in menopause
Menopause is a natural process, not a disease “ which makes words like “symptoms” problematic. But the mental and physical discomforts women are experiencing are very real. Many women experience symptoms so dramatic they’re having a real impact on their quality of life.
Fatigue led the list for our sample, with 85 percent reporting experiencing the exhaustion that isn’t relieved by more sleep. Of those, 66 percent said fatigue interfered with quality of life.
Mood changes, particularly irritability, anxiety, and depression were close behind, with 80 percent reporting experiencing one or more mood impact and 69 percent saying mood issues affected their quality of life.
Sleep disturbances affected a whopping 78 percent of our respondents, and more than half of those said interrupted sleep impacted their quality of life.
More than half surveyed also reported impacts from menopausal belly fat, menstrual issues (usually heavy and/or frequent periods), night sweats, hot flashes, musculoskeletal changes like joint pain, loss of libido, digestive difficulties, and menopause brain fog.
What do we do from here?
Menopause is a thorny problem. Because it varies from woman to woman, even hour to hour within a single woman, “solving for menopause” resists any one-size-fits-all answer. But there are obvious steps we can take to help make women’s lives easier.
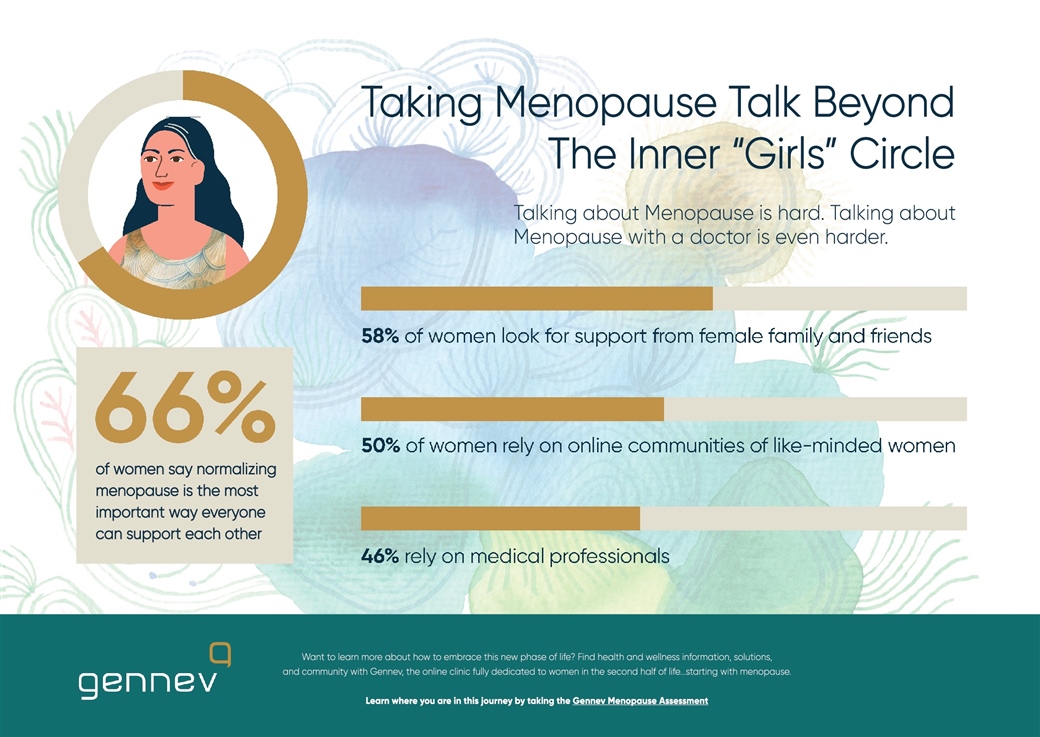
- Normalize menopause. Some are ready to share their #MyMenopauseStory with the world; others would just like to be able to experience a hot flash without feeling embarrassed, but regardless of degree, the majority of our surveyed women think society should regard menopause as the normal, natural, nothing-to-be-ashamed-of process that it is. Why is this so important?
- Research causes and solutions. Because what isn’t seen is rarely studied. We do a lot of research on menopause at Gennev, and the sheer volume of “we don’t know why this happens,” and “medical science isn’t entirely sure why this works,” and frankly, shrugging going on is infuriating. Realizing how many women’s lives are “interrupted” to greater or lesser degree by their symptoms is an important step towards pointing more research in the direction of understanding and helping.
- Get informed. Not only did women want their medical professionals to be better informed about menopause, they felt it would be helpful if their partners had more information. One big call-out from the survey: “don’t take my menopause symptomspersonally.” Forty-six percent of our women wanted their partners to understand that irritability wasn’t necessarily (entirely?) about them; 43 percent would like their partner to be more educated; 38 percent would appreciate more patience.
- Help. Other challenges that women could use help with were balancing work and life (44 percent) and prioritizing self-care (38 percent). Those who wish to help a menopausal woman thrive could do so by helping relieve some of the external pressure: offering flexible work schedules and menopause-friendly offices and taking on more of the burden of housework and care giving could go a long way to making a menopausal woman’s life better.
Thriving now, preparing for later
Lack of information isn’t just inconvenient: it can be dangerous. We were surprised by how relatively few women were concerned about the risks of heart disease, osteoporosis, and Alzheimer’s disease.
Deaths from osteoporotic hip fractures outnumber deaths from breast cancer, yet only 16 percent of those surveyed reported bone density as a concern. Cardiovascular health likewise was low on the list at 23 percent.
Because the choices women make in perimenopause and early post-menopause can have profound impacts on long-term health, we want to begin educating and preparing women now.
So what are we doing? Gennev continues to offer more and more for women in menopause: a network of menopause-specialist physicians and coaches, products that actually help relieve symptoms, a robust and growing community of women and their supporters, and information that’s vetted by medical professionals, so you know you can trust it. And we’ll continue to accrue data to help bring about more research, more understanding, and more solutions.
As Jill Angelo, CEO and co-founder of Gennev, puts it: “Our goal in releasing this data is to reduce the stigma around menopause, help women understand that they are not alone, and to create support systems at home, work, and in healthcare.”
In January, Gennev will release its 2020 Guide to Menopause, a resource women and those who appreciate them can use to understand menopause and its challenges. With more statistics like the ones above, plus tips on managing symptoms and building a healthy foundation for the rest of your life, the 2020 Guide to Menopause will help you thrive through the transition and beyond.
“Not everything on the backside of your body that hurts is menopause lower back pain or spine.” So says our friendly Doctor of Physical Therapy, Meagan Peeters-Gebler PT, DPT, CSCS, CMTPT.
Tailbone pain, “lower back” pain often “¦ aren’t. That pain that’s somewhere in your lower-back-upper-butt region is likely caused by problems with the sacrum and the sacroiliac (SI) joint being irritated.
It’s super common and so we thought it’d be super useful to ask our DPTs to fill us in on the sacrum and SI joint.
If you have problems with sacrum pain, a Gennev menopause-certified gynecologist can give you a trusted opinion, determine if medication is right for you, and they can provide prescription support. Book an appointment with a doctor here.
What is sacrum pain and why does it hurt?
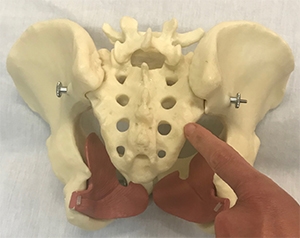
Says Meagan, the sacrum is a triangular-shaped bone that sits just below your lumbar spine and just above your tailbone. Hooked to it on either side are the wing-shaped ilium bones (the knob of your hip bones are at the front of these). The bit that hooks the ilium to the sacrum is your SI joint. Your spine stacks on top of the sacrum.
The spinal column ends above the sacrum but the nerves continue down and through the sacral bone in the form of the cauda equina, a bundle of nerves that resemble a horse’s tail (hence “equina”). The nerves that poke through the middle holes of the sacrum bone feed the pelvic floor, so the system is all pretty intricately linked.

The wedge-shaped sacrum sits within the ring of the pelvis and is intricately controlled by the glute muscles (or what causes knee pain in women) and the pelvic floor. The pelvic floor attaches on the inside of the sacrum and the pelvic ring and is part of the base that provides structural stability to the pelvic ring.
Problems here can be kind of a chicken-and-egg thing, says Meagan. When there’s trouble in the sacral world, it can make pelvic floor problems as pelvic pain, incontinence, and prolapse as worse. Additionally, weakness in the pelvic floor can make the sacrum vulnerable.
Unfortunately, given its shape and location, the sacrum can be vulnerable in women who have poor pelvic strength and health.
Learn how to ramp up your exercise “ safely. Consult with one of our Health Coaches via Gennev HealthFix.
How do I know it’s my sacrum that’s hurting?
Before you start treating the pain, it’s useful to be sure what’s actually hurting and why. So, how do you know what’s hurting?
According to Meagan, sacral pain is usually acute, sharp, and localized in one area. It’s often caused by an action such as bending forward (especially if you do a lot of repetitive bending), or by “asymmetrical” body positioning, like bending and twisting or bending and lifting.
Think about how you get out of your car or how you reach for something in the bottom drawer of your desk while you’re working. Do you turn your whole body first, then bend? Or do you twist part of your body and lean?
The pain is often localized to the thick, broad ligaments on the back of the sacrum. These ligaments have pain fibers in them, so pain might be from the disruption of those tissues or from muscle spasms across the buttock in the piriformis muscle. If the sacrum isn’t moving symmetrically and through its full range of motion, things can start to spasm.
How does my sacrum contribute to incontinence?
According to Meagan, “When the pelvic floor muscles are stuck in spasm, they lose their ability to act like a trampoline and rebound and react to the pressure from the inside. And a spasming muscle is weak because it doesn’t have the right blood flow; it’s not contracting and relaxing properly.
“Plus the pain often makes people hold their breath, and incorrect breathing is itself a major risk factor for pelvic organ prolapse. In this case, it’s causing more pressure in a system that’s already failing.”
What are we doing that causes sacrum problems?
A lot of it comes down to sitting too much and not exercising correctly.
Sitting makes hip flexors really tight, Meagan says. The hip flexors travel on the front of the sacrum, giving a structural tug, repeatedly, in just one direction.
And we strengthen the wrong muscles with popular exercises (we’re looking at you, crunches) because we’re not including the pelvic floor or breathing appropriately or safely. Says Meagan, we get too tight from sitting and we’re too weak in the muscles that need to be strong.
How can we prevent SI or sacrum pain?
There are things we can do to prevent this very literal pain in the butt:
- Be mindful of sitting posture as don’t slouch.
- If you’re sitting a lot, change positions often.
- When exercising, strengthen the right muscles: core work should focus on breath and pelvic floor to be sure both are correct.
- Use a lumbar roll for your sacral pain when sitting.
- Because she usually see problems with forward bending, reaching, rotating, twisting, Meagan suggests you learn to hip hinge and squat appropriately so when you do bend down, you know how to move your hip in the hip socket, rather than dragging the hip, pelvic, sacrum, and spine all together.
When you bend incorrectly, the sacrum becomes the hinge/pivot point rather than the hips, which is not how the body was designed, Meagan says. Hips are more able to move freely and accommodate the load.
Meagan suggests that women imagine they’re wearing a very mini miniskirt and there are lots of paparazzi around. How would that change how you exit your car, for example? Swivel as don’t scissor.
And when you stand, have equal weight on both feet, not an asymmetrical distribution of weight with one hip flung out, for example. And protect your back by using the right movements: when you’re sitting at your desk and want something in a low drawer, pivot your entire body to face the drawer, then bend to retrieve whatever you want. The idea is to move your body in one plane of motion at a time, rather than twisting in more than one.
And your folks were right: don’t slouch. When you slouch, your sacral bone can disengage from the formation of bones and ligaments slightly, and that makes it more vulnerable to injury from sudden or repetitive movement. When we sit up tall, our spine and sacrum stack neatly, as nature intended.
What if I’m already hurting?
Most important, says Meagan, is not to assume you know what’s hurting, because sacral and SI joint pain are often mistaken for something else. Get to an expert physical therapist or chiropractor for a proper diagnosis.
Next, you’ll want to work on freeing things up and getting normal mobility in the joint and area. Then focus on building core strength properly, with the right breathing, and incorporating your pelvic floor and gluteus maximus.
Too often we just assume back pain is an inevitable part of getting older. Not so! say our PTs. By being conscious of posture, by exercising correctly and nixing bad breathing patterns and habits, we can do a lot to protect our backs.
A big thank you to Meagan Peeters-Gebler PT, DPT, CSCS, CMTPT. for her insights.
Have you been diagnosed with a sacrum or SI joint injury? What did you do to rehab it and prevent recurrence? Share with us in our community forums.
Authored by Sports Dietitian, Exercise Physiologist and Gennev Health Coach, Stasi Kasianchuk
Holiday Season is here once again! A time of social gatherings, celebrations, travel, and busy schedules.
Let’s face it, routines can be difficult to stick to during the festive season, especially when it comes to exercise. This is a time of year when many throw their exercise routine out the window and say, “I’ll start again come January!” But if you’re a woman in menopause, movement is especially important for your continued good health.
Why moving is important in menopause
During menopause it can be particularly important to maintain an exercise routine. With the normal decrease in estrogen that occurs during this time of life women are at an increased risk for cardiovascular disease. Maintaining any type of movement supports your cardiovascular system.
Additionally, regular movement can help you sleep better, as well as better manage holiday stress and anxiety which can be further exacerbated during menopause. Finally, with weight management being more of a challenge during this time of life, keeping activity going throughout the holidays can play an integral role in supporting a healthy weight for you.
While exercise may be more of a challenge to fit in (or less of a priority), it does not mean it can’t exist. It may just look a little different than it does most of the year, which the month of December does for most people any way!
Keep moving through the holidays
Here are some simple strategies to stay moving or even start a movement routine during this time of year.
- Plan ahead week-by-week or day-by-day. Set aside time to take a look at your schedule and intentionally block off time to exercise. Doing this for the week can help you be strategic about getting your exercise in. If your week has a lot of tentative plans, it may be best to assess each day at a time. Take a moment in the morning (or the night before) to schedule your exercise time for the day ahead.
- Treat yourself! Give yourself an early holiday gift of a pack of classes you can use at an exercise studio you love or have been wanting to try, so you look forward to it. Buying 5-10 classes that have flexibility in when they are used allows you to book the classes based on your schedule. And packs often end up being cheaper than if you paid per class. Buying several also provides accountability around exercising more frequently in December.
- Break it up and be creative! Traveling, hosting guests, and committing to obligations can all make it challenging to have a large amount of time to dedicate to physical activity. However, even bouts of ten minutes provide cardiovascular benefits. If you have a layover in the airport, take a ten minute (or longer) walk around. Try picking up the pace to increase your breathing and heart rate. If you have a carry-on, getting your heart rate up may be easier than you think. Another option is to park farther away from the store when shopping or take a ten-minute walk before and/or after you shop. It all adds up, and something is always better than nothing!
- Make it a family affair. Include family members in your activity by going for walk to check out holiday lights in the neighborhood after a meal or planning a hike or snow activity with everyone. For some friendly competition, see who can accumulate the most steps each day you are together and award a prize.
- Be kind to yourself. It’s the holidays after all. No reason to beat yourself up if your activity or workout plan did not happen as intended. First assess if there is an abbreviated option you can still do to get some movement in your day (see #3). If the reality is that it just did not happen, rest assured that there is always tomorrow and another opportunity to move. Use it as motivation to start fresh the next day.
Maintaining an activity routine, even if it is different from what you are used to, will make it more likely you will resume your routine in the New Year AND you can continue to get the health and wellness benefits of exercise all month long.
If you haven’t been moving as much as you like and were thinking of starting in 2020, here’s your opportunity to finish strong in 2019 and get a head start on 2020.
Want more strategies on starting or maintaining an exercise routine that is personalized to you? Join the HealthFix program and work with a Gennev Health Coach to get expert support to create a plan that’s best for you.
Tell us what has worked for you to keep moving, or share the challenges you face in the holidays (or any time!) in our community forums.
About Coach Stasi: As a Sports Dietitian, Exercise Physiologist, and endurance athlete, Stasi Kasianchuk has expertise both personally and professionally in using exercise and nutrition to optimize health and performance, and she’s putting that expertise to work, helping women in menopause live their best lives. During her free time she enjoys trail running, cycling, swimming, backpacking, or group fitness classes. Exploring farmers markets, local farms and restaurants and cooking and baking at home also bring her joy.
Sara, 51, shares about how her skin has changed and become drier, thinner, and more sensitive as she started getting perimenopause symptoms:
I had no idea this skin change started in my 20’s.
But it was true. Estrogen, the regulator of many elements including collagen and other body oils, began decreasing the collagen production in my body in my mid-20s, as it does for most women.
Did I notice it then? Nope.
It definitely became noticeable in my 40s when my skin felt”¦ thinner. There was more sensitivity both on my face and all over my body. There were even a few breakouts. At 50, I began to notice and experience dry skin for the first time in my life. My skin had, for most of my life been, been normal-to-oily and was now regularly dry. This was the new normal, and it was baffling and a little surreal, actually.
How can we as adults best care for the 8 lbs and 22 square feet of birthday suit we wear daily? More specifically, how can we better retain or support the moisture content in our skin at every stage of our amazing lives, including menopause?
First things first: hydration and moisture
“Hydration and moisture are not the same things,” shares skin expert and CEO of Teadora Beauty, Valeria Cole.
Drinking good clean water throughout the day is fantastic and will flush and support your system, but it won’t also do the job that a good topical moisturizer can accomplish. Both hydration and moisturization are needed, daily.
In giving yourself the menopause gift of both, your present and future self will thank you. Who knows, you might even enjoy both hydration and moisturization as some of the highest forms of simple self-care tasks you can practice.
Dehydration in menopause can make menopause symptoms worse such as hot flashes, and headaches. If you stay hydrated, you can reduce urinary urgency and bladder irritation (yes, really!), plus a few other benefits. If you’re experiencing night sweats or hot flashes, chances are good you’re losing more hydration with these symptoms, so drink up.
Steady topical moisture and sunscreen to clean skin provide protection and comfort for dry, sensitive, thinning, or itchy menopause skin. Consider testing and investing in a few options:
- A spray mist moisturizer: Which could also feel fantastic on your neck, upper back, decollete, as well as your face during a hot flash, right?
- A good quality serum: Gently press and massage a little oil-based serum (one with some good fatty acids) into freshly cleansed skin, then go straight to your…
- Rich and emollient night moisturizing cream: Massage this gently into your skin and enjoy soft, dewy skin night and day.
- Day time moisture: Once you’ve washed and showered, consider applying the serum again before your regular day time moisturizer. Don’t forget, you’ve lost moisture just by breathing, and then more from night sweats or hot flashes.
- Sunscreen: Have you considered a tinted sunscreen? It does double-duty as a foundation and sunscreen.
- Vaginal moisture support: Delicate and ever-changing, could your most intimate skin tissues use some extra, gentle moisture? Chances are good that you’d feel more comfortable, and experience fewer”¦ ahem, distractions (and itchy sensations) with a little bump of regular topical moisture.
Remember, this is about protection, comfort, and support for a hardworking, ever-renewing, ever-changing, many-layered organ: your gorgeous skin.
Cleansers and washes
A gentler approach may be preferred for more sensitive skin at this time in your life. Facial washes and cleansers without harsh ingredients at this time, please. And this goes also for body washes and exfoliants as well.
Re-framing exfoliation
Cole mentions a helpful term replacement: think “buff,” instead of “scrub”. This is another prompt for gentleness. And frankly, another opportunity for massage. Slow, steady, rhythmic, massage-like buffing paints a much different picture than a quick shower and scrub.
Have you ever been short on time and rubbed really hard in an effort to get clean, fast? Perhaps the water was just a touch too hot in an effort to further speed the process? We’ve all been there, but the results of this may feel harsher, and more painful later on in the day if we’ve scrubbed too hard, or if the water’s been too hot.
Perhaps this is an opportunity to reframe exfoliation in a way that will support ourselves in the body, but also in mind? What if this gentle cleansing and exfoliation time was practiced with more of a massage-like approach? This could be a meditative time for deeper breathing, slow and steady movements, appreciation and gratitude. A ritual to cleanse, wash away, and then replenish.
Elapsed time? 5-8 minutes, includes:
- a gentle facial wash
- exfoliation ritual
- pat dry with a soft towel
- serum massage
- and then night moisturizer massage
Got another 5 minutes for yourself? Take it, indulge, enjoy.
Your skin is an amazing organ in your body, and it works, regenerates, holds us through all of life’s experiences. Not all of it is fun, but we’re all pretty fortunate to be here. Take good care and enjoy good comfort in your beautiful skin.
There’s a whole community of women who are experiencing perimenopause and menopause symptoms like Sara’s in the Gennev Community Forum. Join us, share and comment as a welcome member today.
With so many menopause symptoms, and some of them pretty unpleasant, it can seem like the end of your world. Or at least your world as you knew it.
Amanda Thebe was a lifelong athlete and fitness enthusiast, but when she hit perimenopause at 43, things went … awry. Fatigue set in, and she found her previously boundless reserves of energy were drying up. And, like so many of us, she didn’t realize right away that the issues she was having were hormonal.
And like many women, she ran a gamut of doctors who never even suggested perimenopause. Nausea, vomiting, and extreme fatigue led to dozens of tests (even the emergency room!) over nearly two years.
Menopocalypse Author Interview With Amanda Thebe
Fortunately, at a standard well-woman check up with an OB/GYN, the doc was able to diagnose perimenopause after about five minutes of conversation. A few minutes more, and she had some next steps to start feeling like herself again.
Her book Menopocalypse is Amanda’s way of bringing attention to the fact that women need information and, once they have it, they can actually thrive through this change.
Listen to the podcast, read her book, then check out her website, fitnchips.
TRANSCRIPT TO FOLLOW
Are you feeling like perimenopause or menopause are the end of the world? Talk with other women and women’s health professionals about how they’re surviving their own personal “menopocalypse” in the Gennev Community forums!
I’m a day late with this week’s blog, because I was holding out for Gennev’s latest review of our Menopause Assessment data.
If you’re not familiar with Gennev’s Menopause Assessment, it’s a free questionnaire that, when completed, explains where you’re at in your peri/post menopause journey. You’ll receive a snapshot of how your symptoms compare to our global community of women, plus recommended educational resources, products and a direct connection to a telemedicine doctor for quality care.
We recently reached 5000 completions! This is a fabulous milestone for women’s menopausal health.
With every assessment completed, we’re able to deliver more effective menopause solutions for women like you. The symptom data you share helps us correlate when and how severely symptoms are impacting women of various ages, regions, ethnicities as all with a mission to return more effective solutions to you.
We don’t share this data with anyone. It’s safely collected and secured within our HIPAA compliant system.
Here’s what we’ve learned
68% of you are in perimenopause and 32% in post-menopause
The top 3 highest-reported symptoms are:
Hot flashes are synonymous with menopause, yet only 65% of you reported having them (ranking 9th out of 16 in our symptom categories).
Trusted facts about HRT and effective nutrition are two of your top requests.
Many of you are resourceful when it comes to symptom management. You’ve shared the products, services and behavior changes that have worked for you, which help us recommend solutions to others with similar symptoms. For example, magnesium is one of the most effective dietary supplements you report for trouble sleeping, anxiety and pain management.
Here’s what we’re doing with that important information.
As the largest, most comprehensive database of women’s menopausal data, Gennev is bringing personalized solutions to you.
How many of you read the book, What to expect when you’re expecting? I have never birthed a child, but I’ve given the book to a handful of friends as they embark on the path of motherhood.
Having a baby has a roadmap that’s standard for most women as you know that you will go through the first trimester, the second and third trimesters as and your baby (and body) will transition through phases of growth.
With menopause, the path for every woman is frustratingly unique. You find yourself asking your mother or close friends what the hell is happening in your body. Sadly, we have little to go on when it comes to preparation or even prevention of the symptoms that come with it. And it can be painfully lonely.
Gennev is using the Menopause Assessment data to help us create a menopause roadmap for you. We believe that if we study hundreds of thousands (even millions) of women in peri and post menopause, we can collectively predict where your hormonal health is headed and how it may impact long-term conditions like osteoporosis, heart-health and Alzheimer’s.
The key word here is “collective.”
The more women who take the assessment, the more effective our personalized menopause roadmap will be for every woman who takes it. The more effective the roadmap, the more impactful our services, products and programs.
If you’re one of those women who think you’re “too far gone” beyond menopause, think again. Your post-menopausal symptom reporting informs our ability to bring prevention and behavioral recommendations to you based on what you reported.
Haven’t taken the Menopause Assessment yet? Here’s the link to do so. It takes 7 minutes of your time, but you will come away more informed and resourced than when you started.
If you’ve taken the assessment, thank you. Now, please forward this email to others for our collective power to be realized.
This is a crowdsourcing effort to better healthcare for women in the second half of life. We’re creating a better menopause experience not just for ourselves, but for our daughters and granddaughters and the women who are maturing into some of the best years of their lives.
Let’s do this!

P.S. Happy Labor Day weekend! I’m jetting off to a week of creativity and relaxation with my husband and friends. I’m taking the week to re-energize my brain, my soul and my body and will be back online the week after!
In her own words, guest blogger Anne Miano tells us about learning to be her own best health care advocate.
I got a call one evening last August from my physician’s assistant, who announced, “You need to get to the emergency room for an ultrasound. It looks as though you have ovarian cancer.”
“You need to get to the emergency room for an ultrasound.
It looks as though you have ovarian cancer.”
I’d been suffering from a bloated stomach for several weeks and assumed it was a digestive problem. But an x-ray revealed that I had a large sack of fluid in my abdomen, coming off my right ovary. The radiologist who’d examined my x-ray had made a note in my file that it looked like cancer.
Science has made enormous strides in the past 20 years, and the survival rate for women who’ve been diagnosed early with ovarian cancer is 90%. But for those of us who remember Gilda Radner, who died three years after her diagnosis, and Madeline Kahn, who died a year after hers, “ovarian cancer” sounds like a death sentence.
Stunned, I drove myself to the hospital, sat in the waiting room, and thought about all the things I needed to do to prepare myself and my family for the journey ahead. After I was called into an examination room, I was met by an ER doctor who told me that x-rays aren’t conclusive. But after I got the ultrasound as which did give me the opportunity to experience the notorious vaginal probe as she told me, “I have bad news.” She said I would have surgery within the week, so I called my parents in New Jersey to tell them I probably had cancer, and they made plans to come to Seattle for the surgery.
All the people diagnosing me as except for the oncologist as
didn’t know what they were talking about.
At this point, I’m going to go ahead and reveal: I did not have ovarian cancer. For almost two weeks, I thought I did, but when I met with a gynecology oncologist to go over all my tests, she said, “There’s a 90% chance the mass is benign.”
So how did we go from one person saying she was nearly certain I had cancer to someone else saying she was nearly certain I didn’t?
Here’s the terrible answer: All the people diagnosing me as except for the oncologist as didn’t know what they were talking about.
I grew a suspicious bag of goo
I had developed a 6.5-pound Mucinous Cystadenoma. (My translation: “a big bag of goo.”) It’s not a rare type of ovarian cyst, but it’s not common, not like fibroids, and it comprises only about 15% of ovarian cysts. My guess is that when the radiologist and ER doctor saw a large liquid mass in my abdomen, they assumed it was ovarian cancer because they knew fluid in the abdomen was one of the symptoms. But with ovarian cancer, I’ve since learned, the fluid is usually loose, not contained in a sack.
The doctors who jumped to “ovarian cancer” probably had never encountered a Mucinous Cystadenoma, so they based their assessments of my condition on what they had seen, what they knew from their experience, that fluid in the abdomen equals cancer. But the gynecology oncologist, who was also my surgeon, had seen and removed hundreds of goo bags just like mine. She knew immediately what kind of cyst I had and that there was a relatively low probability as around 10% as the mass was malignant.
Doctors aren’t all-knowing or superhuman
I haven’t known many doctors in my life, not personally, so for me, they’ve always carried a kind of mystique. I grew up believing, because of their education and intelligence, that doctors have nearly magical powers. They solve mysteries and save lives. They’re experts who know my body better than anyone. And so when a doctor tells me something, I believe it.
Or, rather, I used to.
What I’ve learned through my experience is that doctors are people, just like me. The knowledge they carry has been gathered through education and experience. They diagnose based upon what they know, but they don’t know everything.
Every person who told me I had ovarian cancer did so with compassion and a genuine concern for my welfare. They didn’t speak to me with arrogance or dismissiveness. They showed a sense of urgency and believed they were doing what was best. Even so, they failed to provide me with great medical care because, first, my health care cooperative didn’t have a protocol for dealing with cases like mine as or if they did, they didn’t follow it; and, second, because I completely handed over control of my medical care to people I didn’t know and allowed myself to be bounced from doctor to doctor without ever demanding that I be given a clear plan for my diagnosis and treatment.
In hindsight, I messed up
I try not to regret all the times throughout this misadventure when I abdicated responsibility for myself and allowed strangers to have dominion over my body. But I have them, regrets, and they’ve reshaped how I think about my health care.
A year ago, I was having cramping in my right ovary, and I made an appointment for a pelvic exam. My doctor, a woman for whom I have enormous respect and appreciation, had recently left the health care cooperative, and I’d been assigned to a new doctor, a man. I hadn’t had a male doctor in twenty years, and I didn’t want one. Rather than make appointments with him, I’d gotten into the habit of seeing his physician’s assistant, whom I’d gotten to know when she worked for my previous doctor.
First regret: I should have gotten myself reassigned to a woman doctor, someone with whom I was comfortable. But I didn’t. And when the cramping started, I made an appointment, as usual, with the PA, who examined my ovaries and said everything seemed fine. I left the appointment, had a couple more cramping incidents, and then forgot about the problem, because the pain went away.
Second regret: When the PA said she didn’t see anything wrong, I should have asked for a referral to a gynecologist. I had never had an issue with my reproductive system. Not a yeast infection, an abnormal pap smear, or even a late period. And so I assumed, because the PA didn’t see anything, that I was fine. In fact, having cramping like that between periods, when I’d never had it before, was a sign that, for the first time, I wasn’t fine, and I needed to see specialist.
Third regret: I should have trusted the messages my body was sending me, rejected the assessment “nothing’s wrong,” and pushed to have an ultrasound. But I didn’t. By the time my next symptom appeared as the bloating as my cyst was huge, and removal required a nine-inch vertical incision up my abdomen.
Fourth regret: I didn’t choose a quarterback.
Fourth regret: I didn’t choose a quarterback. As soon as I got the cancer call from the PA, I should have contacted my doctor. Even though I didn’t know him, I should have met with him in person, insisted that he take charge of my case, and ask him to walk me through the diagnostic process. Instead, I allowed myself to be passed around from PA to radiologist to ER doctor to lab technician, without ever having a clear understanding of what information needed to be gathered, how it would be gathered, who would analyze it, and who was responsible for explaining the results to me. The radiologist looked at the x-ray. The ER doctor looked at the ultrasound. But it wasn’t until my oncologist got involved, after nearly two weeks of chaos and terror, that someone reviewed all the test results and explained to me what they meant:
Here is what we know. You have a large mass of fluid, but it’s contained, not loose, and all your blood work shows that everything is normal. You haven’t been losing weight, you don’t show markers for ovarian cancer, and there’s a high probability the mass is benign.
That is information, real information, delivered in a professional, respectful, balanced manner. Everything that had come before my meeting with the oncologist had been nothing more than speculation.
Shame on my health care cooperative for allowing so much speculation to be shared with me. And shame on me for not putting a stop to it.
I wrote some New Rules
All my life, because I’d never had a health issue, I’ve been passive about my medical care. I’ve trusted and listened too much, questioned and demanded too little. But I’m done with that approach.
I’ve set New Rules for safeguarding my health:
- I am queen of my health care, the only queen of my health care, because no one knows my body like I do. I am in charge.
- If I have pain, something is wrong, and I won’t allow it to be dismissed as “nothing.” I will ask for additional tests and make an appointment with a specialist.
- I will maintain a relationship with my primary care physician, require him/her to be my quarterback, and explicitly task him/her with guiding me through the testing and diagnosis process.
- I will reject speculation and only accept diagnoses from doctors who have been assigned that duty, rather than from medical professionals I happen to encounter along the diagnostic path.
- I will put aside the lessons I’ve been taught since I was a little girl as to accept without question the opinions of experts, not to be pushy, and not to demand more than I’ve been given as and I will act, instead, as a woman who knows and is confident in her worth, her intelligence and her body.
The first step in implementing these New Rules was to get a new health care team.
After my surgery, I called the health care cooperative to make a follow-up appointment and said I didn’t want to see my primary care physician. I wanted a different doctor, a woman, and I told the scheduler which woman doctor I wanted to see.
When I met the doctor, I sat in a chair across from her and said I needed to go over a few things before I was willing to get on the examination table. I told her my story as of the cancer speculation, the lack of follow-up from my doctor, and how scared and alone I’d felt.
“I want to be clear about what I expect of you as my doctor,” I said. “Because I won’t allow this to ever happen again.” I laid out my New Rules and finished with, “I need you to be my quarterback. If you can do that, I’d like you to be my doctor. If not, I’ll find somebody else.”
“If you can do that, I’d like you to be my doctor. If not, I’ll find somebody else.”
“I can do that,” she said.
I climbed onto the examination table and showed her my scar.
“Which one is the “sandwich generation’?” you may well be asking.
Simply put, it’s those folks who are parents or guardians to kids and caregivers for parents or elder family members, whether they are living in the same house or not.
What else is happening? For those with female reproductive parts, the stages of perimenopause/menopause may be entering the picture as well.
If you waited a while to have or adopt kids, and you’ve got elders in your life or family who are living longer, this kind of life and living could be part of your future as well.
Coordinating childcare and eldercare while navigating menopause is no joke. And many people are entering this very life, while also buying groceries, working full-time (or more than full-time), running businesses, and whatever else they can fit in.
Think about it, even if this isn’t you right now”¦ This would be 3 three different developmental stages of life, each with their own needs, appointments, nutrition needs, and preferences, not to mention mental and emotional needs and support.
“Sandwich generation”… the term isn’t exactly new
Dorothy Miller coined the term in the early 80’s to describe women in their 30s and 40s who were taking care of their aging parents as well as their young children.
According to Pew Research Center (2012), roughly 47 percent of adults in their 40s and 50s have a parent who is 65+ and are raising at least one young child or financially supporting a grown child (18+). Primetime for perimenopause and menopause, right?
Where are you on your menopause journey? Take the Gennev Menopause Assessment.
Taking your time, and taking you-time
Being between two generations in need of care and support can take a real toll on body, mind, mindset, and wellness. Taking the needed time and energy for your own care, feeding, hydrating, wellness, sleep hygiene, and just plain being is critical.
Perhaps this can be simpler than you think. Could 2-3 minutes of doodling while you listen to a favorite song you haven’t heard in ages help you unwind without making you unravel? Could mixing your own decade-of-choice playlist for a little while give you a sense of fun and creativity?
What about staring out the window for a few minutes? Give yourself the luxury, and needed few minutes, to do nothing.
Self-care, whether it takes a lot of time or a very little, may be a hard habit to cultivate. You may not even feel good about taking the time, energy, or steps out the door if you’ve been a caregiver for someone who has gone through a severe illness or who is recovering in your home from a surgery or procedure.
Guilt may show up in the face of you doing something like taking a walk by yourself. You may need to exert yourself to take this kind of care of yourself. This is common and shows up for many people, and it’s going to give you more energy and focus when you do it.
Menopause provides all kinds of symptoms to experience life in; we share about many of them several times each week: anxiety, depression, hot flashes“¦ anger and rage. They aren’t fun, but they are real. This may be similar to many of the caregiving tasks you may be faced with.
Include yourself, even in a small way, and especially if you don’t feel you have the time or energy, in your caregiving.
This is not a time to “just do it”
Doing it, whatever “it” is, yourself may seem like the easiest thing to do in the moment.
This can also be habit-forming, give an illusion of having control, and ultimately be quite isolating, as well as serving as a fast-track to burnout. Remember, you’re going through your own changes as you’re experiencing perimenopause symptoms.
Engaging in help, support, and resources from other family or community members may take time and feel challenging, but doing it alone for years (or even decades), won’t serve. It can be difficult, even painful, to ask for help and support, but truly, it’s needed and worth it for the long game. After all, we all need help sometimes.
A few ideas to get you started
- Gimme a “No”… NO! One thing to remember, “No” doesn’t mean “Never.” Or, if you’re really uncomfortable with that, how about a strong “Not right now”? Or, “not today”? We can do it all and have it all, but maybe not all at once.
- What can they do? Kids and elders may be more willing to help than you think. Ask about it, talk about it. And if you’re very brave, and it’s appropriate, let them know that you’ve got a struggle or two and could really use some help.
- Get specific. Jot down a list of “It’d be amazing if”¦” Just have the brainstorm, make the list, and give yourself the opportunity to see what can happen, who may show up, and how you could be helped. Here’s the thing”¦ you’ve got to be open to both identifying and also receiving the help or solution to have that amazing thing happen. A few suggestions of specifics:
- Regular laundry service for your dad
- Friday night game night for family and a few close neighbors, including potluck dinner
Map out your plan to manage menopause with a Gennev Health Coach
Body transformation, loss, and more change
This is a rich time in life: transformation, change… and more change. There’s plenty to navigate in caring for others, plus the myriad changes in your body as you journey through menopause. Care and attention must be spent on your body’s and mind’s wellness and health.
Emotions around loss, challenge, and change can pile up. Kids are growing up and moving away, parents or elders may be experiencing various forms of decline or aging, your own body’s estrogen levels are diminishing, and the reproductive organs are closing up shop. This is a high volume of change. Personal change.
Support is key. So, look around, ask around. Who else is going through this? Who “gets it” in your world?
More about living than anything else
When you step back and look at what’s going on in your body and in your life, how do you want to “be” with those you love most in the world? How do you want to feel? How do you want to live? What do you want your health and mindset to be? And what are you willing to do to achieve what you want and need for yourself and your family? This is now the game of life. You can build one you’ll enjoy living with those you love.
What are you experiencing as a person caring for kids and elders? Where are your biggest challenges? And where are you finding your most surprising wins? Please share your insights, and scoop up a few of ours, in the Gennev Community Forums.