Culturally, we have this idea that life slows at 50. Children are grown and gone, we’re looking into retirement, our days of doing new things and surprising ourselves are over. Life past 50, if you look at the marketing for this age group, is mostly about fear: fear over health, fear over finances, fear of the future.
Nothing could be further from the truth, says David Stewart of the AGEIST. People in the 50-plus age group are doing all sorts of amazing things. Women especially are “figuring out life 2.0,” says David.
AGEIST’s message is that culture and brands really misunderstand this age group “ it’s not a time of fear, and messaging to the 50+ that way won’t resonate with a lot of the over-50s. Many in this cohort feel “at the peak of their powers,” David says, and if you want to reach them, you need to understand that.
Interview with David Harry Stewart the founder of AGEIST
David Harry Stewart is the founder and face of the AGEIST and the host of the SuperAge podcast. He is a passionate champion and leading authority on the modern 50+ lifestyle, and the mindset and aspirations that drive this influential demographic. Prior to launching AGEIST, Stewart enjoyed an award-winning career as a photographer whose advertising work included Nike, Google, American Express and others, and his magazine work includes Esquire, GQ, Interview, RedBull, Time, and many others.
Hear his conversation with the online menopause clinic, Gennev CEO Jill Angelo, as they discuss our cultural assumptions about aging, how men and women seem to enter the second half of life a little differently (at least at the moment), and what life after 50 really can look like.
Are you past or approaching 50 and feeling the cultural assumptions David and Jill talk about? Or do you think times are changing, and we face aging differently now? Join us in the Gennev Community forums to talk further!
“Is dizziness a symptom of menopause?” We get this question a lot. As well as how to stop heart palpitations from hormones , electric shock sensation, and changes in body odor–all odd, yet real menopause issues–yes, we’re here to tell you that some women may experience menopause dizziness during this life transition.
And we’re going to tackle the who, what, when, where, and why of this particular symptom so that, should you encounter it during your perimenopause or menopause experience, you’re armed with information and ready to take control.
Different Types of Dizziness
Did you know there are three different types of dizziness? It’s true!
First, there’s lightheadedness, where your head likens itself to a balloon whose ribbon has just been released. This sensation can often be accompanied by clouded vision, the feeling that you may faint, or a loss of balance and fall.
Second up is disequilibrium. Defined by the Merriam-Webster Dictionary as a “loss or lack of equilibrium,” this is the type of dizziness where you feel as if you’re about to fall, or the floor is tilting, and not in a fun way. Other symptoms that can occur during an episode of this type of dizziness include unsteadiness, spatial disorientation, and faintness.
Last, but not least, there’s vertigo. Is the room spinning? Are you feeling pulled in one direction or like you could fall over at any moment? That’s vertigo for you. This form of dizziness can often bring with it headaches, sweating, ringing in the ears, and vomiting.
If any of the above three types of dizziness occur, lie down and wait for the sensations to pass. Once you’re feeling steady and able to safely move, get up slowly and start hydrating. Then? As always, we prefer being safe rather than sorry, so call your doctor and schedule a time to check-in.*
What Causes Menopause Dizziness?
As with many perimenopausal and menopausal symptoms, there’s often not one answer to what causes certain symptoms. But we’ve gathered some possible suspects.
Hormonal changes
You’ve likely heard a lot about the impact of hormonal changes during perimenopause and menopause. In a word? Huge. At a certain point in your life, your ovaries stop producing eggs. This causes the body to slow down the production of estrogen and progesterone. It’s the lesser amount of these two hormones that lead to all kinds of menopausal symptoms, possibly including dizziness.
Menopause and blood sugar
Menopause and blood sugar don’t mix well. Our friends estrogen and progesterone also dabble in regulating your blood sugar. So, when the body produces less and less of these two hormones, fluctuations in your blood sugar can occur, likely leading to dizziness in some women. This is why you need a good understanding of hormones and nutrition.
Middle ear issues
Not to repeat ourselves, but HORMONES. Changes in estrogen and progesterone can impact your inner ear health. The inner ear can be impacted by tinnitus in menopause and the inner ear health is vital to balance. Balance is key to staving off dizziness.
Fatigue
A very common symptom for older women in menopause is fatigue. Unfortunately, it can seriously impact you and your body in a variety of ways, including, for some women, sleep disturbances, mental menopause brain fog, mental lapses, and, wait for it–dizziness.
Migraines
One of the most common complaints during perimenopause, migraines can be triggered by hormonal changes–and even worsen headaches during menopause. And one of the aspects of experiencing a migraine? You guessed it. Dizziness.
Aging
Obviously not exclusive to menopause, but intimately tied, aging in general has been linked to dizziness–and more so in women than men. Some studies suggest an increase in the likelihood of experiencing vertigo as you age/go through menopause. That is why if you are older than 40, we advise you to get a menopause test done.
But this is definitely one of those areas where more scientific study is needed to provide concrete proof.
Metabolism
The process that the body uses to convert the food and drink you consume into energy, metabolism during menopause slows down due to a decrease in estrogen and muscle mass. Less estrogen can negatively impact blood glucose levels. And as those levels rise and fall, it’s possible that your cells will not receive the energy they need. This can cause dizziness.
Ways to Treat Dizziness
We’re going to provide a few lifestyle changes here, which you should read, think about, and consider incorporating into your daily routine. And then, you should see your doctor. We’re big on that because, well, that’s what they’re there for.
Stay hydrated
Are you tired of being told to drink water? Staying hydrated in menopause is honestly one of the best things you can do for your body. And if you hate plain water? Try squeezing some fresh lemon or orange juice into your glass. And there’s always decaffeinated herbal tea. Also, track your water intake. There are all sorts of ways to do this–special glasses that measure out exactly how much you need daily and apps for not only adding “drink water” to your to-do list, but recording your progress.
Reduce stress
With menopause and stress…this is easier said than done. Work, family, finances, illness, loss–we’re right there with you. But the truth is, the stuff that triggers stress is never going to magically disappear. So it’s time to take a proactive stance. Exercise. Meditate. Improve your diet. You don’t have to do everything at once. And let go of any ideas you might have that once you introduce stress-relievers into your life, you’ll become a zen goddess who never, ever experiences stress again. This isn’t Disney. It’s your life, and there will continue to be ups and downs. But maybe, the ups start to outweigh the downs, and you’ll see what a life with less stress really has to offer.
Snack
It can feel counterintuitive to encourage snacking because menopausal weight gain is so common. After all, it’s harder for a perimenopausal or menopausal women to lose weight. So shouldn’t we be eating less, rather than more? Not exactly. The trick is to eat the right foods, especially when it comes to regulating your blood sugar–which is important in warding of dizziness. Choose snacks made up of unsaturated fats such as nuts, avocados, flax seeds, and green veggies. And avoid the saturated and artificial trans fats found in many processed baked goods and snack foods. Say goodbye to french fries.
Here’s To Treating Menopause Dizziness
At the end of the day, dizziness is not typically a sign of something more severe,* which is a good thing. But we know this doesn’t make it any less annoying. Hopefully, the combination of knowledge, some new lifestyle choices, and a check-in with your doctor will make you feel more in control of your dizziness. You’ve got this.
*It is not Gennev’s intention to provide specific medical advice, but rather to provide users with information to better understand their health and their diagnosed disorders. Specific medical advice will not be provided, and Gennev urges you to consult with a qualified physician for diagnosis and for answers to your personal questions.
Experiencing dizziness? We’d love to hear about your experience, so please share in our community forums, on our Facebook page, or in Midlife & Menopause Solutions, our closed Facebook group
Have you taken our menopause assessment? Join over 100,000 women to learn more about your symptoms and where you are in the menopause journey.
Learn about Gennev’s menopause blog information from the founder herself, Jill Angelo.
What are the “Menopause Types” and why are they important?
As we explained in last week’s blog, Type 1 & Pre-menopause is where it all begins. Many women aren’t even aware of what’s happening “ or that anything is happening “ in the early part of Type 1. By the time she hits Type 2, she’s aware that something is happening, and she doesn’t care for it!
It’s important for every woman to know what’s happening in her body so she can respond appropriately. Can you imagine being 11 or 12 and having cramps and bleeding without knowing what a period is? Why should a woman in menopause be in the dark about the changes in her body?
Type 2: Stay calm and learn about your hormones
Every woman has the right to know where she is in the menopausal journey.
Especially the Type 2s. But because we don’t talk about menopause, women are frightened of what’s happening, thinking something is terribly wrong. It’s not, of course: it’s the utterly normal and natural process of menopause.
In Type 2, even though they’re in the thick of it, many women still don’t realize their physical and emotional changes are related to their hormones. If women are waiting for that first hot flash to tell them they’re in menopause, they may miss a lot of symptoms that can tell them sooner.
Also, some perimenopause symptoms “ in all types, but particularly in Type 2 “ can be truly frightening: anxiety risks, panic attacks, heart palpitations, flooding periods. Understanding that these happen can help so many women avoid unnecessary fear and ER visits and get to the right treatment faster.
Our Chief Medical Officer goes over the Symptoms and Science happening in Type 2 in this instructional video.
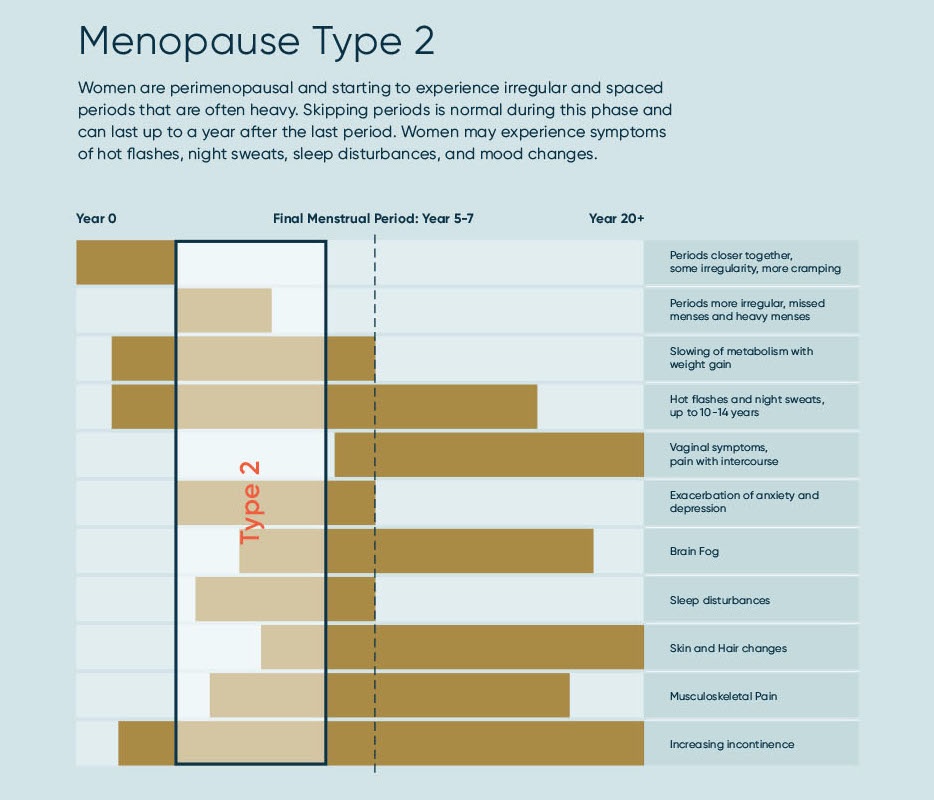
We created a “bird’s eye view” of where you are in your menopause journey and what to expect as to the ebb and flow of symptoms through the different menopause Types: where are you in your menopause journey.
{kind=link}
Type 2 Symptoms
It’s no wonder women are confused: who would associate knee pain or heart palpitations with hormones? But because we have estrogen receptors all over our bodies, the effects of estrogen withdrawal are widespread, causing symptoms from brain fog to plantar fasciitis.
So let’s verify what Type 2 can look like as estrogen and progesterone start ramping downward.
Menopause Type 2s, your common pain points are:
- Irregular periods, often spaced farther apart, sometimes skipped, and probably heavier than usual.
- Further slowing of metabolism, with weight gain, often in the belly.
- Hot flashes start or may increase in frequency and intensity.
- Anxiety and depression can occur, reoccur, or worsen.
- Brain fog, memory lapse, and difficulty focusing can happen as there’s less estrogen to the brain.
- Sleep disturbances can start or increase.
- Skin and hair changes may begin with drying skin; brittle, thinning hair, and wrinkles.
- Joint pain increases, frequently showing up as knee and hip pain, pain in the hands, back pain, though pain can occur nearly anywhere.
- Increasing incontinence.
What to do about menopause in Type 2
First and foremost, start managing your symptoms. Type 2 is, in many ways, the most challenging phase with the greatest number of symptoms, often at their greatest intensity. Don’t just suffer! Since fatigue and sleeplessness are bad enough on their own and can make All The Things worse, we strongly suggest our Gennev AM/PM System. The multi-vitamin pack helps you have energy and balance during the day; and our sleep supports are formulated to help you fall asleep, stay asleep, and wake without anxiety.
Have you tried Jill’s Daily Vitamins for better sleep, focus, and energy?
Are you craving the energy you used to have? We’ve designed this daily menopause pack to help restore energy during the day and improve sleep at night.
This is a good time to be tracking your symptoms and looking for triggers. Recording what you eat and drink, when you exercise, how often you pee, etc., may help you determine what triggers hot flashes, night sweats, urgency incontinence (that feeling that you’re not going to make it to the bathroom on time), poor sleep, and more.
You also want to start building your team. This can include a menopause-specialist OB/GYN, a pelvic Physical Therapist, a Health Coach, and your support squad of friends, family, and community. Sound crowded? It doesn’t have to be. Since estrogen decline affects you head-to-toe, shouldn’t your team cover you head-to-toe?
Finally, don’t panic. This phase can be challenging, but there are treatments to help you get through it, healthy and well. Find good, trustworthy (physician-vetted, if possible) information to understand the changes and know what to expect. Consider sharing information with your family and friends, so they can be better supports for you. And definitely consider sharing with younger women, so they have the knowledge they need, right from the start.
This can be a healthy, even wonderful, time of life. Seek help when you need it; it’s here for you.
With it being Pride Month, I thought I would broach the topic of menopause and identity.
Happy Pride Month in celebration of our LGBTQI+ community!
My mind is on the topic of menopause every day. As we enter Pride Month, I searched on stories about how LGBTQI+ people experience menopause. Just like other phases of our reproductive health, starting with menstruation and moving through menopause, I can’t help but think that identity adds another layer of uniqueness”¦and loneliness.
I’ve mentioned before and I say it again, we are masters at masking our trek through menopause. But consider if you had another layer of covering that masks your day-to-day? Identity as whether you identify as straight, gay, transgender, ***, inter-sex or gender-neutral as complicates how you show up.
Most recently, I read Bunny Cook’s article in Hello Magazine titled “The menopause and me as when you’re gender neutral.” We’ve all felt invisible at times, but Cook’s comments about the lack of menopausal health information and how it’s portrayed in the media made me pause when she stated,
“”¦a bit of information targeted at me, people like me, might have helped. It might have helped show me the way, from puberty to menopause, and educated me a bit more as and made me loathe my truth a bit less.”
A few months ago, genneve’s private Facebook community Midlife & Menopause Solutions welcomed our first transgender male. We didn’t know how a community of self-identifying women would welcome someone who identifies differently yet experiences the same hormone-inducing changes that the female reproductive system naturally goes through.
If you’ve ever had a warm, nurturing hug that almost brings you to tears, that’s what it felt like. This community showed up, and I was in awe of how everyone embraced him because we all had one thing in common: menopause.
Whatever you believe or identify as, I sincerely hope you will take pause to consider every person in menopause who is celebrating Pride Month. If you don’t agree or have more to add, you know I love honest feedback and conversation. Email me jill@gennev.com.
Stay tuned for next week’s blog which will reveal your responses to last week’s post on What do we call “women in menopause”? In hindsight, I should have broadened it to What do we call “people in menopause.” #imlearning.
Stay chill. Happy Pride.

As a a consulting psychologist, consultant and executive coach to high-achieving women, guest blogger Barbara Mark, PhD, knows something about the storms of midlife. Here she takes on the six conditions of the perfect midlife storm and tells us how to survive the weather.
“Midlife: when the Universe grabs your shoulders and tells you,
“I’m not f***ing around, use the gifts you were given.'” “ Brené Brown
If you are a woman in your late thirties to your late fifties you are entering into, are in the middle of, or are coming out of the perfect storm.
Yes, there’s an “out” to this storm, and you’ll get there. I promise.
Not all women experience this storm with the same intensity, as we are all different with different backgrounds and different communities. Your experience may be that of a squall, or you may find yourself holding on for dear life in a Category 5 hurricane. (If that is the case for you, my heart goes out to you!)
The elements that make up this perfect storm are
- The Stages of Adult Development
- The Happiness U-Curve
- The Social and Economic Realities
- Perimenopause
- The Sandwich Experience
- Cultural Beliefs About Midlife
First of all, it is important to know that you are not alone, you’re in good company. All women are subject to these factors to varying degrees, but we all go through it.
If you need help riding the menopause wave, then a Gennev menopause-certified gynecologist can give you a trusted opinion, determine if medication is right for you, and they can provide prescription support. Book an appointment with a doctor here.
The Stages of Adult Development
Although it wasn’t until the 1950s, 60s, and 70s that psychologists began to recognize how adults go through stages just as children do, my favorite theorist, Carl Jung, developed his theory of adult development in the 1920s and 30s. Jung experienced a spiritual and intellectual crisis after Freud ended their friendship and professional relationship around 1915. He later identified this time as a spiritual crisis in the middle of life. In 1965, psychologist Elliott Jaques coined the term “mid-life crisis.”
Not everyone experiences a “crisis” as such as it depends on how intense your perfect storm is.
I love this topic and could go on for pages, but let me say simply that the stages of adult psycho/social development that occur in an individual’s 30s, 40s and 50s are the most tumultuous.
Why? Well, we move from a relatively happy young adulthood through deciding that we don’t want to follow anyone else’s rules or meet others’ expectations, to discovering that there is a self to embrace, only then to encounter fears that this self may not be all that our younger self imagined and wanted to be when it grew up. This leaves us feeling, “Is this all there is?” until finally we arrive at a place of self-acceptance in our mid-to-late-50s to mid-60s.
For many women, midlife means an increase in anxiety, depression, and rage. But it is, like adolescence, a transitional (and hormonal!) phase with an ending. The important thing is to find tools (hobbies, exercise, family and friends) that will help you get through to the good stuff on the other side. Trust me as the post-menopausal zest and the last stage of midlife development are awesome! Then adult development goes on to the stages of older adulthood which are pretty cool, too.
The Happiness U-Curve
In the early 2000s, while everyone was looking at happiness, a few theorists developed and evolved the Happiness U-Curve. It is based on a group of longitudinal and multi-cultural studies of life satisfaction, happiness, and contentment. What the results showed was a curve at high levels of happiness in early life that then dives downward to its lowest level in the late 40s, before climbing back up beginning in the late 50s and early 60s.
The nadir of the curve is just at the developmental moment of greatest self-doubt and the search for purpose and meaning. If you’re feeling at the bottom, as unhappy as you can ever remember being, understand that it’s a curve, and there’s an up awaiting you. By this time your hormones have settled down quite a bit and you are feeling the psychological impact of arriving at big self-acceptance!
The Social and Economic Realities
If you are an American woman in your late 30s through your early 50s, you have lived through some difficult times in US history. Many parents’ child rearing practices were pretty hands-off, thus creating a generation of latch-key kids. There were a lot of divorces. The American economy went from OK to boom to bust to OK to a huge recession to a slow recovery. The recession made it more difficult to embrace the typical American Dream of home ownership and wealth-building.
There are big decisions to be made as Marriage? Kids? Kids before or after marriage or without marriage? Intense career development early on and then take time off from work? Try to get back into work or start an entrepreneurial venture? Try to move the Baby Boomers out of the way while dodging the Millennials who are running up behind and past you? And, this is just a cursory review! Wow, I am exhausted just writing this, yet I know that the economy is better and there are lots of resources out there for you.
Perimenopause
While all this is happening, your hormones are having a party at your expense. Many women begin to experience the first stirrings of hormonal fluctuations in their late 30s. This will continue through to menopause, defined as the point at which you have had no period for one year, around 50-52.
The list of perimenopausal symptoms is long and varied. Many women experience hot-flashes, night sweats, insomnia, mind-crushing fatigue, brain fog, anxiety, depression, heart palpitations, migraines, irritability, crying spells, episodes of rage, and lack of impulse control, to name a few.
If you are still young, preparing for this early in your life as your 20s and 30s as will make the transition a whole lot easier. Dedicate yourself to a good diet and lots of exercise. Develop a routine of mindfulness and self-care so that you are not scrambling to create it when you are in the middle of this.
If you are in the middle of this, contact a menopause specialist and assess the options that are right for you. Also, exercise and mind your diet. This doesn’t have to be hellish even if you are on the more “hurricane” end of the spectrum!
Trust me as this is not your new normal! This party ends and you’ll celebrate being past this ritual of maturation physically, emotionally, and psychologically.
The Sandwich Experience
Many if not most women are caretakers, and if kids are in the picture and parents are needing help at the same time, life can be a sandwich of competing needs and demands. For many women, travel is involved as more family members live some distance away from each other. Also, women who grew up at this time period are less likely to have many siblings that can pitch in to take care of aging parents, so the burden can fall to just one or two people. This, too, evolves. Give it time and give yourself a lot of self-care!
Cultural Beliefs about Midlife
Last but not least is the social construct that midlife equals “old.” In our youth-obsessed culture we have gendered ageism, meaning “old women” become marginalized and invisible.
As a result, so many women are doing everything they can to deny that they are aging and are not speaking up for what they need or engaging in appropriate self-care. Women are running around exhausted and dripping with sweat, trying to prove to themselves and everyone else that they’ve got it all covered.
We are living longer and healthier, so people no longer feel “old” in their 40s, 50s, 60s and for many even in their 70s! However, we have not updated our concept of what the middle of our lives is. The important thing is to live your midlife, not the one dictated by myths and outdated societal stereotypes.
There is calm after the storm
There is “calm” after the storm, if calm is what you want. But there’s also so much more: excitement, change, growth, confidence, and empowerment.
We now can have a midlife that is a productive, satisfying, full third of our lives book-ended by youth and older-age. I meet so many women who say that being in this middle third of their lives is the most empowered and vibrant time of their lives so far. If you met me in my late forties I would say that I was running out of time to accomplish all that I wanted to in my life. Now in my late sixties I am on top of the world and loving my work and my life.
Take heart, women! This can be a difficult and challenging time, but we have so much more access to information and community support from organizations like Gennev than we’ve ever had. Your hormones will settle down, you will move to a place of self-awareness and integration developmentally, and you will move up the other side of the U-Curve! Yippee!
For more from Barbara, check out her blogs on Middlescence and having fun (yes, fun) in midlife.
Weathering your own perfect storm? We’d love to hear about it. Leave a comment below or on Gennev’s Facebook page, or join Midlife & Menopause Solutions, Gennev’s closed Facebook group!
During pregnancy, morning sickness or feeling nauseous affects most women so it gets lots of attention. Not so when it happens later in life. Thankfully, it’s less common and less frequent during menopause than during pregnancy. Since there are so many possible causes of an upset stomach, its connection to this stage of life is probably overlooked. But for those experiencing it, stomach issues can be unpleasant and disruptive.
Why am I experiencing nausea in menopause?
There hasn’t been much research on menopause-related nausea, so the best we have are some educated guesses.
One theory points to the decline in progesterone. Low levels of this hormone and estrogen may contribute to GI troubles. These hormones fluctuate during regular menstrual cycles, so if you’ve experienced nausea related to your cycle in the past or during pregnancy, you may find yourself dealing with it again in perimenopause and menopause.
Nausea may also result from other menopausal symptoms such as strong hot flashes, headaches especially migraines, dizziness, fatigue, anxiety, and heart palpitations. In addition, nausea can be a side effect of some medications like hormone replacement therapy and antidepressants prescribed to help alleviate symptoms like hot flashes.
What to do about feeling nauseous
If you find yourself nauseated first thing in the morning, dehydration may be to blame. If you’re eating too much junk food or not eating enough, low blood sugar levels may be behind your nausea. Here are some more ways to find out what’s upsetting your stomach and calm it down.
Take a pregnancy test. It’s less likely in perimenopause when your periods may be erratic, but not impossible.
Do some detective work. Is there a pattern to your problem? When does it strike? If you’re still having periods, does it happen a few days ahead of your cycle? Does it occur before or after mealtimes? Too much wine, coffee, sugar, and spicy foods may be to blame. Is it related to eating certain types of food? For example, as you get older, your body can have a harder time digesting dairy. Does drinking some water help? If so, it could be dehydration. Is it related to any medication you take? If you can uncover triggers for the nausea, you can avoid or manage them more effectively to get relief.
Look at recent changes. Have you started taking a new medication? Are you eating or drinking something new? Do you have any new stressors in your life? Any changes in your sleeping or eating patterns? If these changes coincided with the nausea, they could be related.
Adjust your eating habits. Limit or avoid spicy, greasy, and sugary foods which can all upset your stomach. Ditto for alcohol, coffee, and any other food triggers that you discover. Eat smaller, more frequent meals, and take your time while eating. Be sure to drink a lot of water during meals, which helps with digestion. Don’t skip meals, even if you’re feeling queasy. Having no food in your stomach may make matters worse, so at least try something bland like white rice or saltines (just like they recommend to pregnant women).
Experiment with relaxation techniques. Before you skip over this tip because you’re thinking “Yeh, right,” or you’re sick of hearing it, there’s some information you may not have heard. Your body has a gut-brain axis, a communication system between your brain and your belly. Because of this connection, stress had been shown to physically alter aspects of your gastrointestinal tract that can result in symptoms like nausea. It could be worth finding a way to ease some of the stress in your life.
Try some spices. Ginger is a popular remedy for general nausea so it might help during menopause too. Other spices that may offer some relief are fennel and cinnamon. They’ve been shown to be effective for relieving pregnancy and menstrual nausea, according to studies.
When to get help for your nausea
Treatment for nausea often requires discovering the cause, so checking with your doctor may offer faster relief. Gastroesophageal reflux disease, commonly referred to as GERD, is similar to heartburn and can result in nausea. Other conditions that can cause tummy troubles are peptic ulcers, diabetes, and migraines.
We can help you remedy your nausea
- Meet with a Gennev Doctor to manage nausea in menopause, and optimize your overall health in post-reproductive years.
- Vitality is our number one daily supplement for women in menopause. It supports mood, energy, stress response, immune health, joint pain, and inflammation.
The information on the Gennev site is never meant to replace the care of a qualified medical professional. Hormonal shifts throughout menopause can prompt a lot of changes in your body, and simply assuming something is “just menopause” can leave you vulnerable to other possible causes. Always consult with your physician or schedule an appointment with one of Gennev’s telemedicine doctors before beginning any new treatment or therapy.
A menopause site might seem like a strange place to introduce the topic of fertility, but it’s surprising how often these conversations overlap, from surprise pregnancies in perimenopause to women who just want to know what the possibilities are after age 40.
Interview with Dr. Lora Shahine of Pacific NW Fertility
Gennev CEO Jill had a chance to sit down with Dr. Lora Shahine, reproductive endocrinologist and fertility specialist at Pacific NW Fertility, to talk about fertility, pregnancy loss, and the options women and couples have to start or complete their families.
01:40
Dr. Shahine explains what a “reproductive endocrinologist” is and why someone might seek out her care if they’re trying to start or add to their family.
02:32
How does a couple know it’s time to visit a specialist? Dr. Shahine explains the impact “Dr. Internet” has had on her practice and gives some guidelines around when it’s time to get help in getting pregnant.
04:54
What are the different fertility paths? How do you choose between IVF vs pills to promote ovulation vs insemination? Dr. Shahine explains both high tech and low tech treatments, as well as how she and her patients determine the roadmap to achieve desired goals.
07:00
How does Dr. Shahine judge where to start with a patient? It starts with the patient’s story from her own point of view as what she’s experienced so far, what she’s tried, what her goals are (soccer team? just one?). Hear from Dr. Shahine how new technologies have opened up lots of new options.
09:25
There are a lot of myths surrounding fertility and how much science can do to promote it. Dr. Shahine gives us the truths around making babies and the wonders as and limits as of technological intervention.
12:34
Making a baby requires having a good egg to start with. Dr. Shahine lets us in on what makes an egg “good.”
13:40
Where do you see innovation? Dr. Shahine explains the importance of mitochondria in reproduction and how new research may allow us to move healthy mitochondria from a young egg into an older egg to give the egg that youthful energy.
14:28
What is it with age anyway? Dr. Shahine explains why Mick Jagger can have a baby at 72 but most women’s peak reproductive years are over by age 40. Hint: it often has to do with chromosome imbalance, and the older the egg, the likelier the chance of miscarriage.
17:29
Dr. Shahine answers those questions you’ve always wondered about: How do sperm die, and what happens to them if they’re not ejaculated? What happens to unused eggs? Why don’t women who’ve been on birth control pills as and therefore not ovulating as have a “reserve” of eggs?
19:40
What about the emotional side? “My job has very high highs and very low lows,” says Dr. Shahine. She explains how she helps women cope with the feelings of shame, guilt, and failure that often (and wrongly) surround miscarriage. There are lots of reasons for hope, she says, and a big part of her job is convincing women and couples to stay positive.
19:50
So, how does she help women stay positive? Dr. Shahine is a huge believer in education and knowledge and grounding hope in the possibilities that science and nature provide. She talks about the importance of self-care and how women so often struggle to prioritize themselves appropriately.
23:41
Does stress affect your fertility? Dr. Shahine wants people to understand that while there is a mind-body connection, stressing about stress is the wrong focus. She gives great tips on how to shift thinking to healthfulness, mindfulness, and being present and positive.
26:39
Dr. Shahine wants to change the conversation from guilt and shame to knowledge, empowerment, and support. Awareness will lead to funding for more research and more innovation around fertility, so it’s important to have open conversations.
29:20
Your takeaway? There’s so much fear and pressure around fertility, says Dr. Shahine, yet there are options for those who are finding it difficult to conceive. Have hope.
You can find out more about Dr. Lora Shahine on the Pacific NW Fertility website or by following her on Twitter: @drlorashahine. Order her book Not Broken: An Approachable Guide to Miscarriage and Recurrent Pregnancy Loss.
This podcast is for any woman over 40 who’s felt invisible or unheard.
Imagine starting a new career at 46 as one that involves putting on bathing suits or lingerie or gorgeous gowns, and getting your picture taken to be in magazines and advertisements and social media campaigns.
It’s hard to be “invisible” when your picture is on the side of a bus!
The Incredible Story Of Rachel Peru
Rachel Peru started modeling at 46. She embraced her silver hair, her body’s natural curves, her newfound “go for it” attitude, creativity or zest, and now she’s traveling, on the cover of publications like Goldie Magazine, and having a wonderful time of it all.

Listen to her conversation with Gennev CEO Jill Angelo about finding confidence and her own voice, how her children feel about their mom’s modelling career, the challenges of being a 40+ model, and the unexpected joys that can come from taking big risks.
Have you embarked on a second (or third or fourth) career after 40? What was it, and what encouraged you to make the leap? We’d love to hear about the challenges and successes, so please share. Tell us your story in the comments below, join the conversation on “second careers” on our community forums, tell us about it on our Facebook page or in our closed Facebook group.
Photo credit: Goldie Magazine, Photographer Steve Cockram @stevieroyphoto.
Thumbnail Image part of the I Am More Than project @iam_more_than. Photographer Matt Brown @mattsphotosuk
Itch, feminine dryness, pain, irregular bleeding: in midlife and menopause and our post-menopausal years, vaginal issues are common, but women don’t have to live with the discomfort and inconvenience. And we shouldn’t as some vaginal issues, like bleeding after menopause, can be indicators of more serious conditions.
We asked board-certified OB-GYN and Gennev Chief Medical Officer, Dr. Rebecca Dunsmoor-Su, to help us identify some of the common concerns, explain what’s happening, and let us know what we should be doing next.
If you have additional questions, please contact your own doctor (especially if urgent), or send us an email at info@gennev.com, and we’ll follow up with Dr. Dunsmoor-Su.
We could also connect you to a Gennev menopause-certified gynecologist to give you a trusted opinion, determine if medication is right for you, and they can provide prescription support. Book an appointment with a doctor here.
One: What are the most common vaginal issues women experience in menopause?
Well, that is a good question. First of all, no two women are alike. What I find as a physician is that the experience of menopause is different for everyone, even though I may be seeing very similar signs when I do an exam.
With that being said, I find the most common complaint I get is vaginal dryness. Women find that they feel dry day to day, sometimes with lichen sclelerosis to flare up or itchiness. They feel dryer during intercourse and sometimes even lubricants for sex aren’t enough to help with that feeling.
Along with dryness I see a lot of women who have pain with intercourse. These two things are related, and are due to the change in the mucosa of the vulva and the vagina with the reduced estrogen circulating. I find that women who have an abrupt shift into menopause (either due to surgery or breast cancer treatment) often have the worst of these symptoms. This may be due to the abrupt change instead of gradual adjustment.
Do you experience pain with sex? Discover causes and solutions: watch Gennev’s how to avoir painful sex webinar.
Things that women don’t realize are due to the vaginal changes as but which can be very bothersome as are urinary symptoms. This can be due to the overall changes in the vaginal mucosa which leave the urethra (the tube that carries urine from the bladder to the outside) or the bladder itself unsupported. Frequent UTI or urinary infections can also occur due to the change in the bacteria that live in the vagina.
Vulvar conditions
Rarely there can be additional vulvar conditions that can can exacerbate these symptoms, called can exacerbate these symptoms and Lichen planus, but these are uncommon, and a separate topic.
Want to learn more about overcoming painful sex?
Read Gennev’s tips on how to sex without pain
Two: What exactly is happening? Vaginal changes in menopause
As estrogen levels decline with menopause, the tissues that respond to estrogen all change. We notice the change in the uterine lining because we stop having periods as that lining thins out. The vaginal and vulvar tissues also get thinner as the estrogen goes away.
Before menopause, estrogen causes the layers in the walls of the vaginal to be thick and elastic. There are lots of collagen molecules (giving elasticity), hyaluronic acid, and blood vessels bringing in moisture. Glycogen is created by the cells in the walls of the vagina. Because of the structure of the walls, the top layer of the vaginal wall breaks away on a regular basis, and the lactobacilli (the good guys) eat that glycogen and help keep the pH of the vagina low (acidic). This keeps away other bacteria and yeast.
All of the above things that keep the vagina plump rely on the stimulus of estrogen. Once the estrogen levels drop, the tissues become thinner and less elastic. When we do biopsies, we see very thin tissue with few layers. The moisture, collagen and acid production shrink significantly. Lactobacilli can no longer survive in the vagina, so other bacteria come in and replace them, and these are sometimes not such “good guys.” A lot of women notice increased discomfort and / or decreased sensation due to these changes.
Three: At what point should a woman talk to her doctor about vaginal problems she’s experiencing? Are any of these potentially dangerous?
If the symptoms are bothering you, talk to your doctor. There are many levels of therapy that can be helpful.
If your doctor is uncomfortable talking about sexual or vaginal issues, or does not have specific training in treating women in menopause, an OB/GYN is the specialist you want to see. Our OB/GYN doctors all have hormone and menopause training, though some may have more comfort than others with the topic. When you call, don’t be shy about asking for someone who sees menopausal patients on a regular basis.
Need an expert’s diagnosis? A Gennev menopause-certified gynecologist can give you a trusted opinion, determine if medication is right for you, and they can provide prescription support. Book an appointment with a doctor here.
In general, vaginal changes aren’t dangerous. However, if women simply assume their symptoms are due to menopause alone, they may miss other disease processes. It is especially important to see your physician if you have a history of HPV or abnormal pap smear, as this virus can cause cancer on the outside and in the vagina as well.
As mentioned before, sometimes the irritation is not just menopause but a more severe disorder such as lichen sclerosis, which must be treated to prevent long-term damage. A good exam by an experienced provider can help sort these out.
Four: What should women be looking out for and paying attention to, when it comes to their bodies? Are there early warning signs women should be aware of?
Well, that’s a broad question. It is important to recognize that with menopause our breast size and bodies change with age. While all of the changes that come can be normal, we may not like some of them. Sometimes it is important to recognize what is normal versus what is abnormal, or “pathologic,” as we like to say in medicine.
In terms of symptoms:
- Bleeding after you have had no period for a year (are in menopause) is NOT normal. It can be just due to thin lining or even the vagina, but it ALWAYS needs to be evaluated to rule out cancer.
- Pain with intercourse, lack of desire, changes in sensation in the vaginal region and vulva can all be “normal” but they are not functional and not OK. You should feel free to bring this up with your doctor and have a frank discussion about what can be done to make sure your sex life after menopause or during continues to be an important part of your life and health.
- Day-to-day menopause vaginal itching and dryness can also be normal, but if it is impacting your daily life, it can be treated with multiple different modalities.
- Hot flashes and menopausal night sweats are a normal part of the menopausal transition for some women, but if they impact your life, we can talk about lifestyle changes and treatments that may help get rid of hot flashes and night chills.
Making adjustments in your lifestyle can help you manage those pesky perimenopause and menopause symptoms. Book 30 minutes for your personal consultation with a Gennev dietitian.
Five: Women experiencing menopause in the offices are often embarrassed by the changes in their bodies. How do you put women at ease to have these conversations?
First and foremost you need to be seeing a provider with whom you feel comfortable to have any conversation. Remember, as physicians, we have heard it all! We are not afraid, in general, to tackle difficult subjects. There is no need to feel shame about feeling menopause symptoms in the office.
If you find that your physician struggles with talking frankly about the more sensitive stuff, or has a lack of knowledge about menopause in particular, seek out someone who is comfortable with it, usually an OB/GYN. We talk about sex all the time”¦.
Six: Do you think doctors should ask women about their sex lives, or is it better to wait for the woman to bring it up?
Well, I think we doctors should be bringing it up, but I specialize in menopause and spend a lot of time talking frankly about sex, lube, treatments, and toys, etc. It takes time and research to learn about these things, and many providers did not get great training on how to approach these subjects.
If your doctor isn’t asking, ask them! They can’t help you if they don’t know that sex is an issue.
In “vaginal issues in menopause: Q&A with an ob/gyn (part 2)“ Dr. Dunsmoor-Su takes on treatments (hormonal, non-hormonal, laser therapy), addresses the fears women have about HRT and bio-identical hormones, talks about alternative therapies such as acupuncture, herbs, and OTC remedies, and discusses her thoughts on how doctors should be trained to understand and treat menopausal issues and the women who are looking for help.
If you’re suffering from vaginal issues, don’t hesitate to talk with your doctor. Please don’t use this blog or any similar online resource to self-diagnose: articles such as this should not be considered a replacement for treatment by a healthcare professional.
Have you had vaginal issues? What happened, and how are you putting things right? We’d love to hear from you, so please share in the comments below (you can share anonymously, if that’s more comfortable for you), on our Facebook page, or in Midlife & Menopause Solutions, our private Facebook group.
Wanting to get fit or get more fit is a worthy and admirable goal. But if your goal is truly to be healthier, the average Facebook-fueled “30 days to your best bikini bod” challenge may not be the best way to reach it, especially for women in midlife and menopause.
Bikini Bod Challenge
“Do 30 crunches for 30 days” for rock hard abs, a chiseled physique, buns of steel, etc. We’ve all seen them, maybe thought about joining, maybe even tried one. And they can work. They can also be really physically and emotionally destructive.
In this blog, we’ll tackle the physical issues and how to address them; in part 2 we tackle the emotional concerns and detail the much healthier challenge our DPTs recommend.
Why are challenges so bad?
They’re not all bad. But some can be problematic for your body and your emotional health. To learn more, we talked with those fabulous Docs of Physical Therapy, Dr. Meagan Peeters-Gebler and Dr. Brianna Droessler-Aschliman.
There are several things to be wary of when considering jumping into a challenge, they tell me. Here’s what to look out for:
Dangers to your physical health
The problem: Not enough recovery
According to Meagan, “Muscles don’t function optimally if you bring them to fatigue every single day. When you do strength training, for example, you’re shortening those muscles. They need recovery time to return to resting length. If you’re creating tension over and over and not stretching properly, not resting, then you’re at risk of developing muscular trigger points for pain, or tendonitis, or overuse injuries.”
She continues, “Exercise is cellular breakdown, it’s tearing down the muscle tissue. You need time to rebuild from that as that’s actually when your muscles get bigger and stronger. A day may not be enough time to recover to baseline and be ready to do that activity again. The goal is to make gains in strength, flexibility, and endurance, and you can’t do that if you’re only breaking down, not building up.”
The solution: Give your body time to recover properly
Challenges, unfortunately, can actively (ha ha) discourage proper rest. Often, rest isn’t built into the program. And because participants share their “progress” on social media, we can be motivated by competitiveness or embarrassment to carry on, even when our body is clearly telling us not to.
If it helps, “rest” doesn’t have to mean “do nothing,” our DPTs tell us.
You can choose “active recovery,” in which you do a different activity and reduce your overall level of intensity and exertion. Or you can choose to take a “rest day,” where you may do very little that raises your heart rate.
How do you know what rest you need?
Listen to your body, say our DPTs.
“If you wake up in pain,” says Meagan, “and it’s localized, and the pain gets worse as you do the activity, then that’s a loud, clear message from your system not to do that. If you know you’re getting sick, don’t tax your system. If you aren’t sleeping, take a recovery day.”
Brianna agrees: “If you’re really stressed, that may be a day to rest. But listening to your body is so critical. If you’re supposed to do this thing, and halfway into it, you’re just not feeling it and your strength and endurance are way down, stop. Stop now. That’s one of the problems with challenges as they encourage us to do this thing even when it’s not a good idea today. We worry about failing the challenge or the training plan by not following it perfectly, but it’s OK as it’s smarter, in fact as not to push and increase risk of injury or overuse strain.”
The problem: Too much repetition
Many challenges are single-activity: 30 days of crunches, running every day for 6 months, etc. Coupling repeated motions with insufficient rest is really asking for trouble, say our DPTs.
Says Meagan, “You can be active daily, but you need variability of motion.” That means not doing the same thing, or even similar things, day after day, she says. “Running and biking use mostly the same plane of motion, so that may not provide enough variability, but running and body weight resistance exercises or biking and yoga do. You need to offset the sheer repetition that can cause damage.”
The solution: Mix it up
According to Brianna, “Not doing the same activity every single day is better. Active recovery is fine; you don’t have to do nothing. But don’t do the same activity day after day. Don’t use the same planes of motion every single day, because you’re missing out on other components of true strength and health. Use all the planes of motion to make your whole body healthy and avoid injury.”
You need diversity of activity, but you also need diversity of intensity: harder effort some days, easier others. Challenges that have you do 100 push-ups for 100 days or whatever, don’t give you either.
The problem: Focusing too much on the activity.
One of the problems Bri notices in challenges is they focus entirely on the activity and the number of “reps.”
“But what about the rest of your day?” she asks. “Getting fit isn’t just about the time you’re active. Do you know how to refuel? If you’re not used to this level of activity, you may need to learn how to fuel properly, pre-exercise and post, so you get the nutrients you need and don’t binge eat because you’re extra hungry or feel “entitled.'”
And of course, because many of these challenges are focused on weight loss and appearance, people may intentionally not consume enough calories.
The solution: Make it about a healthy lifestyle
Meagan adds, “Again, it’s about listening to your body over following a schedule. If you’re dehydrated at the end of the day, or you haven’t eaten enough, or you’re tired or stressed, working out in a depleted state just so you can check off that box, is more likely to cause injury than provide benefit. Waiting until the next day when you’re fueled and rested, electrolytes are balanced, you’ve got protein on board, your glycogen is restored, is safer and smarter.”
The trick, say our DPTs, is in adopting a healthier lifestyle that takes everything into account: activity, yes, but also hydration, nutrition, stretching, recovery, and rest. If you’re done thinking about your health before you get out of the shower, you won’t see the results you’re looking for.
The damage a poorly designed challenge can do isn’t just to your body. In tomorrow’s blog, we’ll take on the emotional toll of choosing the wrong challenge for you.
And bonus: Meagan and Bri as both athletes in addition to being DPTs as have some expert advice on how to do it right.
Have you ever done a challenge? Did it work for you? What was it like? We’d love to hear how it went, so let us know in our community forums, on our Facebook page, or in Midlife & Menopause Solutions, our closed Facebook group.
One of the many reasons we love walking for exercise in midlife and menopause is because it is an easy, accessible way for most women to stay active and get outdoors. But what do you do when hot and humid, cold and rainy, or snowy and icy weather keeps you inside? Don’t use it as an excuse to skip your workout!
Keep Moving With An Indoor Walking Workout
Most days, you can make some adjustments, dress appropriately, and weather the storm or the heat. For the days when it’s unsafe or impractical to walk outside, turn to our three indoor workouts that will boost your mood, fight belly fat, give you more energy, and help ease those menopause symptoms. The change of pace will also challenge your body in new ways and add variety to your usual routine. Plus, consistency is the key to seeing results from your exercise efforts.
These three workouts can be done in the comfort of your home (or at the gym) no matter what the weather may be.
Workout 1: The 30-Minute Treadmill Trio
One of the great things about walking on a treadmill is that you’re in command. You control the climate. You can easily walk a precise distance and track your progress. You can add hills when you want them and get rid of them when you don’t. You can multitask while you walk, watching TV, talking on the phone, scrolling social media, or checking your email. Or you can get focused and crank out a heart-pumping, calorie-blasting walk like this one. Adding speed and incline intervals will rev up the fat-burning power of your walk.
Warm-up (easy to moderate intensity)
- 3 minutes: 2.5-3.0 mph, 1% incline
- 3 minutes: 2.8-3.3 mph, 1% incline
- 3 minutes: 3.0-3.5 mph, 1% incline
Part 1: Steady pace (moderate intensity)
- 3 minutes: 3.2-3.8 mph, 1% incline
Part 2: Speed intervals (moderate to hard intensity)
- 1-minute fast interval: 3.5-4.5 mph, 1% incline
- 1-minute recovery interval: 3.0-4.0 mph, 1% incline
- Repeat 2 more times
Part 3: Hill climb burst (moderate to very hard intensity)
- 30 seconds: 3.0-4.0 mph, 2% incline
- Repeat 8 more times, increasing the incline by 1% each time
- 60 seconds: 3.0-4.0 mph, 1% incline
- 30 seconds: as fast as you can go, 1% incline
Cool-down (moderate to easy intensity)
- 2 minutes: 3.0-3.5 mph, 1% incline
- 2 minutes: 2.8-3.3 mph, 1% incline
- 2 minutes: 2.5-3.0 mph, 1% incline
Workout 2: 15-minute High-Energy Indoor Workout
You don’t need any equipment or a lot of space to get an indoor, energy-boosting walk. Unlike walking outdoors, you can safely change the direction and ways your moving”going side-to-side and forward and backward and adding moves like kicks and knee lifts”to work more muscles, which prevents muscle imbalances and boosts your calorie burn. So, turn up your favorite tunes and get moving.
Warm-up
1 minute: march in place
Part 1: Fancy Footwork
- 20 steps marching in place
- 20 heel taps in front of you
- 20 front kicks
- 20 knee lifts
- 20 steps marching in place
30 seconds: walk on your heels with your toes off the floor
30 seconds: walk on your toes with your heels off the floor
Repeat Part 1 one more time
Part 2: Fast Feet
- 20 basic marches in place
- 20 fast marches in place
- Repeat 3 more times
- 20 basic marches in place
1 minute: speed walk around your house, exploring as many rooms as possible
Repeat Part 2 one more time
Part 3: Multi-direction Moves
- 20 side-to-side steps
- 10 rock steps on left foot (step right foot in front of you and then behind you, so you’re rocking on your left foot; each front and back step counts as 1)
- 20 side-to-side steps
- 10 rock steps on right foot (step left foot in front of you and then behind you, so you’re rocking on your right foot; each front and back step counts as 1)
1 minute: climb stairs (no stairs? Step up and down on a single step, exercise step bench, or sturdy low bench, or speed walk around your house again)
Repeat Part 3 one more time
Cool-down
1 minute: march in place
Workout 3: Add 5 Moves for Total-Body Toning
Add these moves to either the 30-minute Treadmill Trio or 15-minute High Energy Indoor Workout. You can turn either of those previous walking workouts into a total body, toning workout by adding our strength moves for walkers. These multi-muscle exercises will build strength to protect your joints, preserve muscle to keep you active, and improve your balance.
Here’s how to do it: After each part of the workouts above, including the warm-ups and cool-downs, do one of the moves in our strength moves for walkers video, completing 10 to 12 reps of each.
For example:
- After you warm up, do 10 to 12 Squats with Heel Lifts before moving onto Part 1 of that workout.
- After you finish Part 1, do Pushups with Side Planks.
- Continue interspersing the moves into the workout you’re doing until you do the last exercise following the cool-down.
- After your workout, finish with a relaxing stretching session to ease tired muscles and improve your flexibility so you’ll be ready to go next time.
Want to get more from your walks? Join the Get Moving Walking Program for Women to receive two 30-day walking programs designed by women for women, support from certified fitness instructors and Gennev menopause specialists, as well as special offers and incentives.
Always check with your physician before beginning any new exercise program.
“At Gennev, we know that being in control” is one of the most important securities that grounds us in life. When you feel in control, it brings contentment. When you’re not in control, things get uncertain and fear and anger often show up.
This week’s events have me feeling uncertain”¦but not without hope.
Whether or not you agree with abortion, the power of government over women’s bodies is once again a hot topic with new legislation in Alabama. I won’t even link to my sources on the new law, because I want to give you the freedom to search out information on the topic that aligns with your views.
Regardless of where you stand on the issue, never would a law be passed holding men to a standard that can change their life forever based on a moment of sex, wanted or unwanted.
What gives me hope is that women (and men) are speaking out about the topic on all sides.
On an equally heavy note, I saw a film titled A Thousand Girls Like Me, in which a 23-year-old Afghan woman speaks out against her father who raped her for 13 years, resulting in countless pregnancies and two children that she is now raising.
Oddly, the story is not as bleak as it sounds. Instead, it’s a story of a young woman using public media to uphold a decade-old law that forbids men from abusing and raping women. The fact that the law is only 10 years old is one issue, but even more, the law hasn’t been enforced until now with Khatera’s brave determination to speak out.
Bringing this full circle, I recently met a woman by the name of Denise Paleothodoros who is speaking out about her rocky start to perimenopause in the work place titled, Menopaused at Work: It Can be a Mind F*ck. In it, she’s honest, she’s funny, she’s human. I loved it, and I love her very real look at how we mask menopause-related symptoms at work.
As women, we’re master cover-up artists. We know how to suck it up when it comes to the pain, embarrassment, and oppression associated with our reproductive health. We’re masters at covering up our angst at being out of control.
But these stories I outlined are examples of women speaking up. They’re paving a path for the rest of us who might not be that bold or aren’t afflicted in the same way, but may know a loved one who has faced unjust ramifications simply for being a woman.
Gennev’s mission is to empower women to take control of their health in midlife and menopause.
Feeling in control starts with knowledge and access to information. It starts simply with knowing where your circle of safety exists, and we hope we can bring that to you.
You don’t have to make a film, march in protest or even bravely publish your story on LinkedIn, but I do encourage you to seek out what makes you feel in control. If you don’t know where to begin, I encourage you to reach out to the Gennev community, ask questions, and experience the power of a people that support you.
Happy Memorial Day Weekend!